Article Text

Abstract
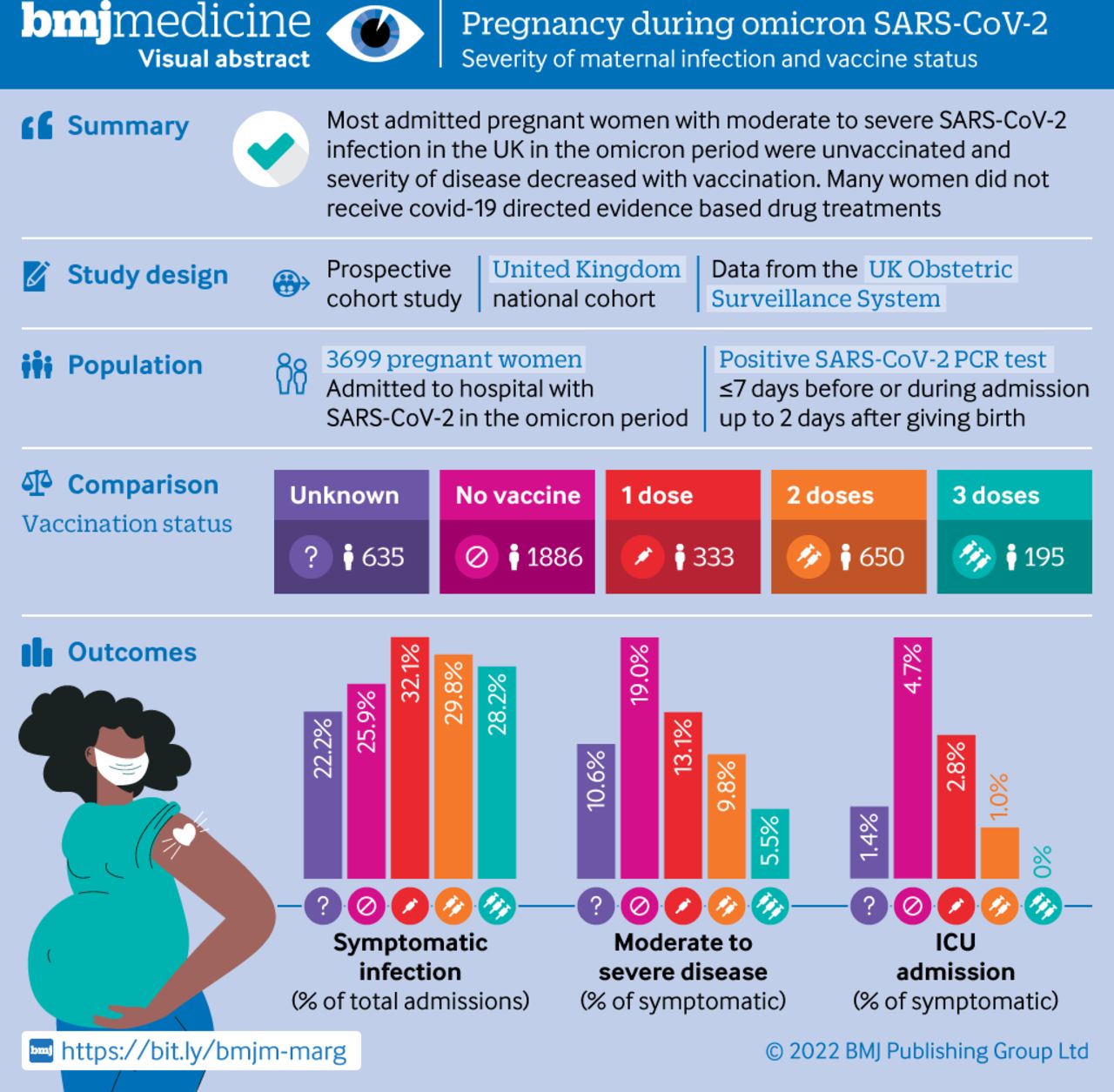
Objectives To describe the severity of maternal infection when the omicron SARS-CoV-2 variant (B.1.1.529) was dominant (15 December 2021 to 14 March 2022) and describe outcomes by symptoms and vaccination status.
Design Prospective, national cohort study using the UK Obstetric Surveillance System.
Setting 94 hospitals in the UK with a consultant led maternity unit.
Participants Pregnant women admitted to hospital for any cause with a positive SARS-CoV-2 test.
Main outcome measures Symptomatic or asymptomatic infection, vaccination status by doses before admission, and severity of maternal infection (moderate or severe infection according to modified World Health Organization's criteria).
Results Of 3699 women who were admitted to hospital, 986 (26.7%, 95% confidence interval 25.3% to 28.1%) had symptoms; of these, 144 (14.6%, 12.5% to 17.0%) had a moderate to severe infection, 99 (10.4%, 8.6% to 12.5%) of 953 received respiratory support, and 30 (3.0%, 2.1% to 4.3%) were admitted to an intensive care unit. Covid-19 specific drug treatment was given to 13 (43.3%) of the 30 women in intensive care. Four women with symptoms died (0.4%, 0.1% to 1.1%). Vaccination status was known for 845 (85.6%) women with symptoms; 489 (58.9%) were unvaccinated and only 55 (6.5%) had three doses. Moderate to severe infection was reported for 93 (19.0%) of 489 unvaccinated women with symptoms, decreasing to three (5.5%) of 55 after three doses. Among the 30 women with symptoms who were admitted to intensive care, 23 (76.7%) were unvaccinated and none had received three doses.
Conclusion Most women with severe covid-19 disease were unvaccinated and vaccine coverage among pregnant women admitted to hospital with SARS-CoV-2 was low. Ongoing action to prioritise and advocate for vaccine uptake in pregnancy is essential. A better understanding of the persistent low use of drug treatments is an urgent priority.
Trial registration ISRCTN 40092247.
- COVID-19
- Pregnancy complications
- Infectious disease medicine
- Public health
- Obstetrics
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
In adults (who are not pregnant), risk of severe respiratory disease with the omicron SARS-CoV-2 variant of concern (B.1.1.529) seems lower than the risk of previous variants
Pregnant women with symptoms who were admitted to hospital when the alpha (B.1.1.7) and delta (B.1.617.2) variants of concern were dominant were at increased risk of moderate to severe SARS-CoV-2 infection compared with when the wild type infection was dominant
Most pregnant women admitted to hospital with symptomatic SARS-CoV-2 infection were unvaccinated
What this study adds
One in five pregnant women admitted to hospital who were not vaccinated had moderate to severe infection, compared with one in 10 with two vaccine doses, and one in 20 with three doses
One in five unvaccinated pregnant women with symptoms who were admitted to hospital during the omicron dominance period had moderate to severe infection compared with one in four admitted during the wild type dominance period
One in ten admitted pregnant women with symptoms needed respiratory support during the period when omicron was dominant and few received covid-19 specific drug treatments
How this study might affect research, practice, or policy
Unvaccinated pregnant women remain at risk of admission to hospital with moderate to severe infection during the omicron dominance period
Ongoing research to assess the impact of new variants of concern and the severity of covid-19 disease in pregnancy is needed
Introduction
In 2020, the World Health Organization’s living systematic review concluded that SARS-CoV-2 infection during pregnancy was associated with an increased risk of admission to intensive care for the mother, increased risk of preterm birth and admission for neonatal care for the infant.1 Included studies initially contained data predominately from the US and China, with few active, population based surveillance studies. The latest update published on 7 May 2022 included studies published before 27 April 2021 and thus comprised mainly of studies of the variants of concern before delta (B.1.617.2).
In the UK, a new SARS-CoV-2 variant of concern (omicron, B.1.1.529) was initially reported 21 November 2021 and was the dominant variant by mid-December 2021.2 Severe maternal infection was more frequent with the alpha (B.1.1.7) and delta variants of concern than with the wild type, and perinatal outcomes were worse.3–5 Most severe maternal and perinatal outcomes occurred among women who were not vaccinated during periods when the alpha and delta variants were dominant.6–8 In the UK, messenger RNA vaccines were recommended to pregnant women from April 2021,9 and in December 2021 pregnant women were recognised as a risk group with priority for vaccination, including a booster dose if the interval from the second dose exceeded three months.10
Initial studies of omicron infection in adult populations (who not were not pregnant) indicated a lower risk of severe pulmonary disease with this variant than with the previous delta variant of concern.11–13 To date, we have not identified any peer reviewed, population based studies exploring the impact of infection with the omicron SARS-CoV-2 variant on pregnant women and perinatal outcomes. Robust national data are urgently needed to inform women who are pregnant or who are planning a pregnancy, as well as health professionals providing care for pregnant women, and policy makers. The primary aim of this study was therefore to describe the characteristics of pregnant women admitted to hospital with SARS-CoV-2 infection including their vaccination status, severity of infection, pharmacological management, and pregnancy and perinatal outcomes, in the period when the omicron variant of concern was dominant in the UK. Figure 1 shows the visual abstract.

Visual abstract. ICU=intensive care unit; PCR=polymerase chain reaction
Methods
Design, data sources, and study period
A national, prospective cohort study was conducted using data from the UK Obstetric Surveillance System.14 This system entails active surveillance with reporting from all 194 hospitals in the UK with a consultant led maternity unit and includes well established routines to secure complete reporting.15 Information about women who died or who had stillbirths or neonatal deaths was crosschecked with data from the organisation responsible for maternal and perinatal death surveillance in the UK (MBRRACE-UK).16 As individual level data for SARS-CoV-2 variants were not recorded in medical records, we restricted inclusion to the period in which the omicron SARS-CoV-2 variant was the dominant circulating strain in the UK (15 December 2021 to 14 March 2022). Pregnancy outcomes were included in the primary report and in supplementary data received by UK Obstetric Surveillance System before 19 April 2022. The start cut-off date of 15 December was chosen because the variant then represented 50% or more of sequenced new infections.13
Study population and study groups
Women were included if they were admitted to hospital during pregnancy and had a positive SARS-CoV-2 polymerase chain reaction (PCR) test in seven days or fewer before admission, during admission or up to two days after giving birth. Hospital admission was defined as a stay in hospital overnight or longer for any cause, or an admission of any duration to give birth. Women who did not meet this case definition were excluded (figure 2). We categorised women who were included into two mutually exclusive groups based on presence or absence of covid-19 symptoms.

{kind=link}
{kind=link}
Inclusion flow chart of pregnant women admitted to hospital with SARS-CoV-2 infection, by admission group in the UK between 15 December 2021 and 14 March 2022
The symptomatic group were women who were reported to be admitted to hospital due to covid-19 disease or symptoms, or who were reported to be symptomatic, or received respiratory support of any kind. The asymptomatic group were women admitted for labour, obstetric care, or other reasons, and who were not reported to have symptoms related to SARS-CoV-2 and who did not receive respiratory support, or who were reported to be asymptomatic if the reason for admission was not known. The vaccination status of these women was categorised by the number of doses before admission: unvaccinated, one dose, two doses, or three doses, or vaccination status unknown.
Measures
A composite measure indicating moderate to severe SARS-CoV-2 infection was based on the WHO criteria of covid-19 disease severity.17 Women were classified as having moderate to severe respiratory disease if one or more of the following was reported: oxygen saturation of <95% on admission, need for respiratory support, evidence of pneumonia on imaging, admission to an intensive care unit, or death. Respiratory support was recorded as the maximum level of support in one of the following categories: oxygen therapy (supplementation by nasal prongs or non-rebreathe mask of <15 L/min), high flow nasal cannula of ≥15 L/min or continuous positive airway pressure, mechanical ventilation, or extracorporeal membrane oxygenation. Mode of birth was categorised as follows: caesarean section before or in labour, assisted vaginal birth, or unassisted vaginal birth. Gestational age was categorised by weeks+days as <22 weeks, 22+0-27+6 weeks, 28+0-33+6 weeks, 34+0-36+6 weeks, and ≥37 weeks for age at admission and age at childbirth. We used the following pregnancy outcomes: pregnancy loss (either miscarriage before 24 weeks or termination of pregnancy), total births, live births, stillbirths, admission to neonatal unit, and early neonatal death in the first week.
The following sociodemographic and medical risk factors were included: maternal age, body mass index, occupation (woman or partner in paid work v neither in paid work), ethnic background (Asian, black, Chinese, other, or mixed ethnic minorities v white), smoking (current smoker v non-smoker), medical conditions before or during pregnancy (asthma, hypertension, cardiac disease, and diabetes before or in pregnancy), parity (nulliparous v multiparous), and plurality (single v multiple). Descriptions of drug treatments were based on national guidance issued on 1 July 2020 using the latest edition at the time of admission.18
The study was registered with ISRCTN (number 40092247) and the protocol is available at https://www.npeu.ox.ac.uk/ukoss/current-surveillance/covid-19-in-pregnancy.
Statistical analysis
Numbers and proportions are presented with 95% confidence intervals calculated by using the Agresti-Coull method, and where data were missing, proportions are presented out of known cases. Statistical analyses were done using STATA version 17 (Statacorp, TX). In this national cohort study, the study sample size was governed by the disease incidence, thus, no formal power calculation was carried out.
Patient and public involvement
Patients and public were part of the UK Obstetric Surveillance System steering committee and were involved in study oversight but not in the design, reporting, conduct, or dissemination of this study. Preliminary results of the study have been published open access on MedRxiv and the final results will be publicly disseminated from the National Perinatal Epidemiology Unit and collaborating organisations.
Results
Of the 3699 women admitted with PCR confirmed SARS-CoV-2 infection between 15 December 2021 and 14 March 2022 (figure 2), 986 (26.7%, 95% confidence interval 25.3 to 28.1) had symptoms and 2713 (73.3%, 71.9 to 74.7) were asymptomatic.
The characteristics of included women by symptom group are shown in table 1. No substantial differences were noted between the groups by age. A body mass index of 30 or more was reported for 30.1% (n=285) and 27.6% (n=719) among women with and without symptoms, respectively. Black, Asian, or other minority ethnic background was reported for 296 (30.6%) women with symptoms and 911 (34.5%) women without. In the symptomatic group, 47.5% (n=461) had a gestational age at admission from 22 to 36+6 completed weeks; this proportion was 21.2% (n=571) in the asymptomatic group. Vaccination status was known for 3064 (82.8%) women, 845 (85.7%) in the symptomatic group and 2219 (81.8%) in the asymptomatic group.
Sociodemographic characteristics and medical risk factors among pregnant women admitted to hospital with SARS-CoV-2, by symptom group in the UK between 15 December 2021 and 14 March 2022
Respiratory support and medical treatment for women with symptomatic covid-19
Nine (0.3%) of 2713 asymptomatic women were admitted to an intensive care unit for indications unrelated to their SARS-CoV-2 infection. Overall, 144 (14.6%) of women with symptoms had at least one indicator of moderate to severe infection (table 2) and 99 (10.4%) required respiratory support. However, the proportion of women with symptoms who received any SARS-CoV-2 specific drug treatment was low (n=50, 5.1%, 95% confidence interval 3.9% to 6.6%); 0.3% (n=3) received antivirals, 0.9% (n=9) received tocilizumab, 4.4% (n=43) received corticosteroids for maternal indication, and 0.6% (n=6) received monoclonal antibodies. Five women were recruited to the RECOVERY trial. Among the 30 women with symptoms who were admitted to intensive care, 13 (43.3%) received specific drug treatment; one woman (3.3%) received antivirals, six (20.0%) received tocilizumab, 11 (36.7%) received corticosteroids for a maternal indication, two (6.7%) received monoclonal antibodies, and one (3.3%) was recruited to the RECOVERY trial.
Respiratory support and medical treatment to pregnant women with symptoms who were admitted to hospital with SARS-CoV-2 infection in the UK between 15 December 2021 and 14 March 2022
Vaccination status
The proportion of women with symptoms who had received no vaccine, one, two or three vaccine doses was 58.9% (n=489), 12.7% (n=107), 23.0% (n=194), and 6.5% (n=55), respectively (table 3). A total of 129 (15.3%) women with symptoms whose vaccination status was known had a composite measure of moderate to severe infection. Approximately one in five (93/489, 19.0%) women with symptoms who were admitted to hospital and who had not been vaccinated had moderate to severe infection, reducing to one in twenty (3/55, 5.5%) among women who received three doses. Of 447 women in the two dose group for whom date of vaccination was available, 353 (79.0%) were known to have received their second vaccine dose more than 3 months before admission; this included 11 (57.9%) of the 19 women who had a composite indicator of moderate to severe infection and two who were admitted to intensive care. Overall, only three (2.3%) of the 129 women who had a composite indicator of moderate to severe infection and known vaccination status had completed the three vaccine doses advised to protect the pregnant population against severe omicron infection at the time of hospital admission.
Outcomes among pregnant women with symptoms who were admitted to hospital with SARS-CoV-2 infection during the period when omicron was the dominant variant by vaccination status in the UK between 15 December 2021 and 14 March 2022
Pregnancy outcomes
Pregnancy outcome was known for 2841 pregnancies, 556 (56.4%) in the symptomatic group and 2285 (84.2%) in the asymptomatic group (table 4). Almost a third of women with symptoms (n=314, 31.9%) were known to have been discharged while still pregnant. The proportion of births at gestational weeks 22-36+6 was 16.0% (n=87) among women with symptoms versus 10.8% (n=238) in women without symptoms. Birth was expedited due to covid-19 for 23 (4.2%) women in the symptomatic group; none of these women was known to have received three vaccine doses (table 5).
Pregnancy outcomes for women admitted with SARS-CoV-2 infection during the period when omicron was the dominant variant, by admission group in the UK between 15 December 2021 and 14 March 2022
Pregnancy outcomes for women admitted with SARS-CoV-2 infection during the period when omicron was the dominant variant, by symptom group and vaccination status in the UK between 15 December 2021 and 14 March 2022
Among 2821 infants, 19 stillbirths were reported; 10 (1.8%) in the symptomatic group and 9 (0.4%) in the asymptomatic group (table 6). Six (60%) of the ten stillbirths among women with symptoms occurred to women who were unvaccinated or had received one dose. From the data available, we were unable to assess the the role of SARS-CoV-2 in the stillbirths. Admission to a neonatal unit was reported for 71 (13.0%) of 549 infants born to women with symptoms and 209 (9.3%) of 2253 infants born to women without symptoms.
Perinatal outcomes among infants of women admitted with SARS-CoV-2 infection during the period when omicron was the dominant variant and who have given birth (n=2821) by symptom group and vaccination status in the UK during 15 December 2021 to 14 March 2022. Data are n (%)
Discussion
Principal findings
This national, prospective cohort study has identified that, among pregnant women admitted to hospital with SARS-CoV-2 infection during the period when the omicron variant of concern was dominant, around one in four were symptomatic. One in ten of these pregnant women with symptoms needed respiratory support. Few women with moderate to severe infection received covid-19 specific drug treatments, notably only around half of the women admitted to an intensive care unit.
One in five pregnant women who had not been vaccinated and were admitted to hospital with symptoms had moderate to severe infection, reducing to one in ten with two vaccine doses and one in twenty with three doses. No women with three doses were admitted to intensive care, and most pregnant women with symptoms and moderate to severe respiratory disease, intensive care unit admission, or who died, had not been vaccinated according to the recommended schedule for the pregnant population for the omicron variant (two doses and a third dose if the interval from the second dose exceeded three months).
Strengths and weaknesses of this study
To our knowledge, this study is the first national, prospective cohort study to describe pregnancy and perinatal outcomes during the period when the omicron SARS-CoV-2 variant was dominant. A key strength of these data is the existing UK Obstetric Surveillance System mechanism for national case identification of all women admitted to hospital across the UK, resulting in low risk of selection bias. Of note, the Obstetric Surveillance System cannot provide information about pregnant women in the general population with mild or asymptomatic disease who are not admitted to hospital. In the UK, universal SARS-CoV-2 testing for all obstetric admissions was implemented from May 2020. Pregnant women without symptoms in whom SARS-CoV-2 infection was detected by screening on admission to hospital, were most commonly admitted to give birth.19 Therefore, we categorised the included women by symptoms to avoid misclassification bias and increased adverse outcomes being incorrectly attributed to SARS-CoV-2.20
Lag periods for vaccines were not included in the current analyses and this could lead to underestimation of protection. Some of the pregnant women who had received two vaccine doses or fewer might also have delayed the second dose due to covid-19 infection; information about previous infection was not available in this study. These women could potentially be misclassified into a category with lower expected protection while having a reduced risk due to post-infection immunity, and this misclassification could result in overestimation of the protective effect of different vaccine doses. As with previous analyses,5 SARS-CoV-2 variant sequencing data were not available for individual women and a proxy time period for the data collection was used instead; this proxy is a limitation. Additionally, more women in the symptomatic group were still pregnant or had not known pregnancy outcome at the latest data retrieval compared with the asymptomatic group, which is likely to affect the observed rates of key neonatal outcomes.
Interpretation and comparison with related studies
In this study during the omicron dominant period, the proportion of women with symptoms and moderate to severe infection was 14.6%, which is lower than in the wild type (24.5%), alpha (36.2%), and delta (42.8%) variant periods in the UK.5 15 However, a greater proportion of pregnant women with symptoms had received one or more vaccine doses than in previous variant periods. This vaccination prevalence needs to be taken into account when comparing outcomes across variant periods, recognising that previous vaccination would likely confer some degree of protection from both severe illness and symptomatic infection. When solely unvaccinated pregnant women admitted to hospital with symptomatic infection are considered, maternal outcomes are similar to those observed during the initial wild type infection period.5 Among those in need of respiratory support, irrespective of vaccination status, the use of mechanic ventilation or extracorporeal membrane oxygenation was 13.3% and thus lower than in previous periods (30.7% in wild type, 23.5% in alpha, and 21.4% in delta periods).5
Covid-19 specific drug treatments, which are now standard care for patients who are not pregnant,21 22 were used infrequently, even for women who needed respiratory support. The proportion of patients that received any drug treatment for covid-19 (one or more of an antiviral, tocilizumab, maternal corticosteroids, and monoclonal antibodies) was lower (5.1%) in our study than in the alpha (14.9%) and delta periods (13.6%). Although this finding might partly reflect a lower severity of illness, only about half of pregnant women admitted to an intensive care unit due to covid-19 received any covid-19 specific drug treatment. The Royal College of Obstetricians and Gynaecologists guidelines issued on 19 June 2020 recommended that corticosteroid treatment should be considered for all women who were clinically deteriorating due to covid-19.18 In our study, maternal corticosteroid treatment was reported for 4.4% of women with symptoms during the omicron period, compared with 12.7% during the alpha and 12.0% during delta periods. Approximately a third (37%) of women admitted to intensive care received corticosteroids.
Few pregnant women who had received two or more doses of vaccine were admitted with symptomatic SARS-CoV-2, and few of the women with a composite indicator for moderate to severe infection had received three vaccine doses according to current recommendations to protect pregnant women against severe omicron infection. Vaccination for all pregnant women regardless of risk group was recommended in the UK from 16 April 2021, and all adults were eligible to receive vaccination from mid-June 2021.23 Pregnant women were identified as a risk group and prioritised for vaccination from mid-December 2021, this included recommendation for a third booster dose if the interval after the second dose exceeded 3 months.10 Vaccine uptake for the second dose by females ranged from 68% to 87% in the age categories from 18 to 45 years in England by 22 May 2022.24 Vaccine coverage surveillance among women who gave birth in England up to 31 January 2022 reported that the proportion of women who had received two doses of vaccine increased from 38.4% in November 2021 to 50.6% in January 2022, while 40.5% were unvaccinated in January 2022.25 Similarly, vaccine coverage has been low in Scotland where 32.2% of women who gave birth in October 2021 had received two doses of vaccine during pregnancy compared with 77.4% of women of reproductive age (18-44 years), and 98.1% of women admitted to the intensive care unit were unvaccinated.6 In the current study, 62% of the women with information about vaccination status were unvaccinated.
In the general adult population, effectiveness against symptomatic disease with omicron variant of concern after the second dose declines from 60-75% three weeks after vaccination to 20% at 15 weeks and 10% after 25 weeks,26 and three doses have been shown to give better protection against severe disease.27 Among women who had received two doses, 79% were known to have received their second dose three or more months prior to admission. The number of pregnant women who had received a third booster dose was low in our study, but few severe infections in this group indicates the importance of the third dose to protect pregnant women from both hospital admission with symptomatic covid-19 and need for respiratory support.
Disproportionate admissions due to covid-19 among pregnant women with ethnic minority backgrounds were less prominent in the current study than previously described during the wild type period.15 National guidance has emphasised the importance of addressing this inequality and advised active healthcare seeking in these groups.18 The observation time in the current study is short and the findings cannot yet reliably indicate if the smaller differences can be attributed to better communication, prevention, healthcare seeking strategies or previous infection. Preliminary surveillance results indicated that the omicron variant of concern has a secondary attack rate of 10-13% and therefore factors that increase transmission, such as multi-occupancy housing and public facing occupations, are important also for this variant.28–30 Since socioeconomic deprivation is also a known independent risk factor for adverse pregnancy outcome, this could be a source of residual confounding in this study.
Neonatal outcomes were purposely not compared between omicron and other periods as a high proportion of pregnancies were continuing at the time of analysis. However, the available data suggest that the risk of stillbirth during this period could be lower than observed during the delta period.5 Further follow-up is required to clarify the effect of infection during the omicron dominant period on perinatal outcomes such as stillbirth.
Implications for clinicians and policy makers
The findings of this study indicate that the risk of severe respiratory failure in unvaccinated pregnant women with omicron variant of concern is similar to that observed in the UK during the initial wild type variant wave of the pandemic.15 Few women with moderate to severe disease received covid-19 specific drug treatments and understanding this persistently low use of evidence based treatments among severely ill pregnant and postpartum women is an increasingly urgent priority.
Although severe outcomes were less frequent in the current period than in the previous alpha and delta variant dominant periods, the risk of hospital admission due to covid-19 was higher in the UK than in other European countries during the initial months of the pandemic.15 ,31 32 This higher risk could be associated with factors such as early implementation of public health measures to limit viral transmission in the other countries. If public health interventions could, to some extent, protect pregnant women during the first wave of covid-19, individual protection through vaccination is now available. Our results indicate that most current instances of respiratory failure among pregnant women are preventable, yet vaccine uptake among pregnant women remains low compared with the general female population of reproductive age. Continued, strong efforts to improve uptake of the vaccine during pregnancy are still needed. This effort is of even greater importance because infection continues to rapidly rise in both high and low resourced settings.33
Data availability statement
No data are available.
Ethics approval
This study was approved by the HRA NRES Committee East Midlands-Nottingham 1 (reference number 12/EM/0365). Individual patient consent for the collection of anonymous data was not required.
Acknowledgments
We would like to acknowledge the assistance of UK Obstetric Surveillance System reporting clinicians, the National Institute for Health and Care Research Reproductive Health and Childbirth National Research Champions, and the UK Obstetric Surveillance System Steering Committee without whose support this research would not have been possible.
References
Footnotes
HME and RR are joint first authors.
Twitter @HildeEngjom, @DrCGale, @Marianfknight
Contributors All authors contributed to the conceptualisation, writing, and editing of this study, had final approval of the version to be published and agree to be accountable for all aspects of the work. KB, EM, NS, CG, PO, MQ, PB, JK, and MK contributed to funding acquisition, supervision, and methodology. HME, RR, NV, KB, and MK contributed to data curation and formal analysis, and had access to verify the underlying data. MK is guarantor of the study. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. Transparency: MK, as guarantor, accepts full responsibility for the work and affirms that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as originally planned have been explained.
Funding The funders had no role in considering the study design or in the collection, analysis, interpretation of data, writing or decision to submit the article for publication.The funders had no role in considering the study design or in the collection, analysis, interpretation of data, writing or decision to submit the article for publication.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: MK, MQ, PB, PO’B, and JJK received grants from the NIHR in relation to the submitted work. HME participated in this work as academic visitor to the National Perinatal Epidemiology Unit with funding from the Norwegian Research Council, grant number 320181, and travel grant from the Nordic Federation of Societies of Obstetrics and Gynecology Research fund, grant number 6302. KB, NV, RR, NABS, and CG declare no competing interests. EM is trustee and president of the Royal College of Obstetricians and Gynaecologists, trustee of British Menopause Society and chair of the Board of Trustees Group B Strep Support. PO’B is vice president of the Royal College of Obstetricians and Gynaecologists and co-chair of the Royal College of Obstetricians and Gynaecologists Vaccine Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability Data cannot be shared publicly because of confidentiality issues and potentially identifiable sensitive data as identified within the Research Ethics Committee application/approval. Requests to access the data can be made by contacting the National Perinatal Epidemiology Unit data access committee via general@npeu.ox.ac.uk.