Article Text

Abstract
Obstructive sleep apnoea is a substantial clinical and public health problem because it contributes to harmful effects on quality of life, daytime symptoms, road traffic incidents, and cardiometabolic disease. Increasingly, obstructive sleep apnoea is recognised as a heterogeneous disease, and patients have varied susceptibility to long term complications and different responses to treatment. This narrative review summarises the current knowledge of precision medicine in obstructive sleep apnoea, particularly the role of symptom clusters, polysomnogram phenotypes, physiological endotypes, and circulating biomarkers in defining subtypes. In the near future, the prognostic accuracy of these measures in predicting long term complications in obstructive sleep apnoea will likely be improved, together with better matching of treatments to disease subtypes.
- Sleep medicine specialty
- Medicine
- Public health
- Therapeutics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Obstructive sleep apnoea is characterised by recurrent collapse of the upper airway during sleep and is the most common respiratory disorder related to sleep.1 Obstructive sleep apnoea is a major global health problem with substantial economic and social burdens because untreated obstructive sleep apnoea is associated with daytime sleepiness,2 poor sleep quality,3 reduced work productivity, and increased rates of road traffic incidents and occupational injuries.4 Obstructive sleep apnoea also causes multiple adverse physiological and biochemical effects, including hypoxaemia, oxidative stress, inflammation, sympathetic activation, cortical arousal, tachycardia, and vasoconstriction. In some patients, these adverse effects cause end organ damage and long term complications, including premature cardiovascular and cerebrovascular disease such as heart attacks and strokes,5 chronic kidney disease,6 and neurodegeneration.7
Precision medicine, also known as personalised medicine, is an approach tailored to the prevention and treatment of the disease that takes into account variability in genes, the environment, and lifestyle for each person.8 Precision medicine targets treatments to patients who are most likely to benefit from them, in contrast with the traditional one-size-fits-all approach for prevention and care. The goal of precision medicine is to target the right treatments to the right patients at the right time.
Obstructive sleep apnea is being recognised increasingly as a heterogeneous disease, and emerging evidence suggests the potential of using precision medicine approaches in its treatment and management.9 1011 12 Patients with obstructive sleep apnoea can be classified into different subtypes based on symptoms, physiology, and molecular characteristics. The purpose of this review was to look at the existing body of knowledge on precision medicine in obstructive sleep apnoea, particularly the potential role of symptom clusters, polysomnogram phenotypes, physiological endotypes, and circulating biomarkers, in helping to define these subtypes. We believe that these factors might help us better understand the pathological basis of obstructive sleep apnoea and its complications, improve the prognosis for the long term effects on health, and better match patients to more specific treatments.
Prevalence of obstructive sleep apnoea
According to a comprehensive literature review from 2019, approximately a billion people worldwide have obstructive sleep apnoea, and 425 million adults have moderate-to-severe disease.2
Sources and selection criteria
We searched PubMed and Medline databases for peer reviewed, English language studies of adult obstructive sleep apnoea, published from 1 January 2012 to 31 May 2022, and manually searched the references of selected articles for relevant articles for our narrative review. We used the following medical subject headings search terms in combination with the term “precision medicine”: “pathophysiology,” “cluster analysis,” “polysomnography,” “biomarker/blood,” “classification,” and “treatment.” We also included highly cited papers published before 2012 based on our narrative review of the literature.
Symptom clusters
A symptom cluster is defined as two or more concurrent symptoms that are related to each other.13 Clinical symptom subtypes are associated with differential risks for prevalent and incident cardiovascular and cerebrovascular disease among patients with moderate-to-severe obstructive sleep apnoea. Ye and colleagues first used latent class analysis, an unsupervised cluster analysis, to identify clinical phenotypes of obstructive sleep apnoea based on symptoms and comorbidities.9 With this data driven approach, they originally explored the differences in the clinical presentation of obstructive sleep apnoea by classifying individuals into three groups: disturbed sleep, minimally symptomatic, and excessive daytime sleepiness. The three clusters were not substantially different for apnoea-hypopnoea index, body mass index, or sex. Most individuals in the disturbed sleep and minimally symptomatic clusters reported classic obstructive sleep apnoea symptoms (ie, pauses in breathing at night and loud snoring),1 14 15 but less often than patients in the excessive daytime sleepiness cluster.9
Symptom subtypes of obstructive sleep apnoea were identified, replicated, and validated based on clinical symptoms in a population based sample of patients with obstructive sleep apnoea.10 Particular symptom subtypes were shown to be independent predictors of prevalent cardiovascular and cerebrovascular disease in moderate-to-severe obstructive sleep apnoea, and an increased risk of incident cardiovascular and cerebrovascular disease among patients with obstructive sleep apnoea (excessively sleepy subtype) was found.10 We and others have identified similar symptom subtypes in clinic based cohorts of obstructive sleep apnoea and have found positive associations between these subtypes and future risk of cardiovascular and cerebrovascular disease.16–18 Although the main limitation is the lack of external validation, other cluster analyses on obstructive sleep apnoea have been published.19
In a 2022 study, subpopulations of patients with obstructive sleep apnoea were defined with latent class analysis in a cohort of Hispanic patients based in the community, and an association between symptom clusters of obstructive sleep apnoea and cardiovascular disease was identified20; the insomnia obstructive sleep apnoea phenotype (apnoea-hypopnoea index mean 10.5 events/h (standard deviation 5.2)) was associated with an increased incidence of cardiovascular and cerebrovascular disease (heart failure, hypertension, and diabetes) compared with those with no obstructive sleep apnoea. Other studies have shown a potential increased risk of cardiovascular and cerebrovascular disease in relation to symptoms of insomnia; for example, in the study by Labarca and colleagues, the disturbed sleep cluster had an increased but non-significant hazard ratio for cardiovascular events (2.87, P=0.11).16 Studies have also reported no significant independent relation between these subtypes and incident cardiovascular and cerebrovascular disease,21 however, and more work is needed in this area to better understand the relation between symptoms of obstructive sleep apnoea and the risk of long term effects on health.
The varied risks of cardiovascular disease seen in these clusters might be relevant when interpreting the results of randomised controlled trials of obstructive sleep apnoea treatment with continuous positive airway pressure. Observational studies have shown a robust reduction in cardiovascular events with continuous positive airway pressure in patients with obstructive sleep apnoea.22 23 By contrast, in large randomised controlled trials, treatment with continuous positive airway pressure did not significantly lower the risk of cardiovascular events in obstructive sleep apnoea. Patients in these randomised controlled trials tended to be non-sleepy, however. For example, in the SAVE (Sleep Apnea Cardiovascular Endpoints), ISAACC (Impact of Sleep Apnea Syndrome in the Evolution of Acute Coronary syndrome. Effect of Intervention with Continuous Positive Airway Pressure), and RICCADSA (Randomised Intervention with Continuous Positive Airway Pressure in Coronary Artery Disease and Obstructive Sleep Apnoea) studies, mean scores on the Epworth sleepiness scale were 7.4,15 5.3,24 and 5.5,25 respectively. The lack of symptoms might have contributed to the low adherence to treatment with continuous positive airway pressure in these trials; furthermore, the selected patients could have had a relatively low risk of cardiovascular and cerebrovascular disease caused by obstructive sleep apnoea itself.26
Physiological endotypes
More precise treatment for obstructive sleep apnoea has been hindered, at least partially, by the lack of an accurate means to assess the pathophysiological mechanisms underlying obstructive sleep apnoea in the clinical setting.27 An endotype of obstructive sleep apnoea represents a subtype that has a distinct physiological mechanism,28 rather than a phenotype which usually refers to the clinical manifestations of the disease.29 The pathogenesis of obstructive sleep apnoea is caused not only by anatomical factors (collapsible or narrow upper airway), but also by potential contributions from non-anatomical factors, such as increased loop gain, reduced pharyngeal muscle responsiveness, and low arousal threshold (physiological endotypes).30 Eckert et al used a three point scale to weigh non-anatomical (muscle responsiveness, arousal threshold, and loop gain) and anatomical (passive critical closing pressure of the upper airway) contributions to obstructive sleep apnoea.31 The study found that 19% of patients with obstructive sleep apnoea had a relatively non-collapsible upper airway similar to many of the control individuals (passive critical closing pressure of the upper airway 22-25 cm H2O) and further highlighted the multifactorial pathophysiology of obstructive sleep apnoea.31
Measuring these physiological characteristics has historically required complex equipment in specialised laboratories, but recent studies suggest that these data might be readily extractable from diagnostic polysomnograms. Sands and colleagues described an automated technique to quantify pharyngeal collapsibility and compensation with diagnostic polysomnographic signals in patients with obstructive sleep apnoea without specialised equipment or interventions.32 Moreover, they extended their approach for estimating arousal threshold and loop gain to evaluate the key traits causing obstructive sleep apnoea, implying that the pathophysiological contributions to the disease can be estimated in the clinical setting.27 33 Finnsson and colleagues reimplemented and validated the methods and algorithms of Sands et al.34 Their new cloud based implementation in Python showed the potential reproducibility and scalability of this approach. These findings could provide access to endophenotyping of obstructive sleep apnoea for more scientists and clinicians, which could then become an integral part of a precision medicine approach to obstructive sleep apnoea.34
Theoretically, treatments could be guided by physiological subtypes. For example, sedatives might reduce the severity of obstructive sleep apnoea in patients who have a low-to-moderate arousal threshold, although this effect is speculative.35 Also, recent data suggest that successful therapeutic responses to currently available treatments for obstructive sleep apnoea might be predicted by these endotypic measurements. Op de Beeck and colleagues used data from diagnostic polysomnography to assess the endotypic mechanisms underlying success versus failure of hypoglossal nerve stimulation (an increasingly common alternative for patients with obstructive sleep apnoea who are intolerant to continuous positive airway pressure).36 Favourable responses to hypoglossal nerve stimulation treatment were independently associated with a higher arousal threshold (odds ratio 6.76, 95% confidence interval 2.44 to 23.3, P=0.001), higher muscle compensation (4.22, 1.70 to 12.55, P=0.004), and a lower loop gain (in milder collapsibility, P=0.003).36
Bamagoos and colleagues performed a secondary endotypic trait analysis of polysomnographic data from patients with obstructive sleep apnoea to find predictors of the efficacy of oral appliances.37 Greater efficacy of oral appliances was associated with particular subgroups of obstructive sleep apnoea (lower loop gain, higher arousal threshold, and lower ventilatory response to arousal), moderate pharyngeal collapsibility, and weaker muscle compensation.37 Op de Beeck and colleagues tested whether endotypes of obstructive sleep apnoea estimated by routine polysomnography could differentiate between responders and non-responders to treatment with mandibular advancement devices.38 Patients who responded to mandibular advancement devices had a significantly lower loop gain (P=0.02), which was calculated from the baseline clinical polysomnogram, consistent with the previous study.37
A secondary data analysis of treatment of obstructive sleep apnoea in patients with acute stroke examined the association between endotypic traits and adherence to continuous positive airway pressure. Decreased arousal threshold and increased pharyngeal muscle compensation were associated with lower adherence to continuous positive airway pressure in patients with stroke, suggesting that these traits might help predict adherence to continuous positive airway pressure.39 Further clarification of specific physiological endotypes in individuals with obstructive sleep apnoea might facilitate the development of new treatments that can be tailored to individual patient needs according to the physiological endotype or endotypes of their disease.
Hence these endotypes could help in identifying patients who might have greater improvements in symptoms and more robust responses to specific treatments for obstructive sleep apnoea. Because of the limitations of using only the apnoea-hypopnoea index as an indicator of disease and its severity (see next section), assessment of endotypes of obstructive sleep apnoea should help to better characterise the heterogeneity of the disease.
Advanced polysomnographic metrics
When obstructive sleep apnoea is suspected, patients will often undergo polysomnography in a sleep laboratory, an overnight study where physiological data are continuously collected over eight hours: electroencephalography (EEG), electrocardiography, oxygen saturation, airflow, electromyography, and chest wall and abdominal movements. Based almost solely on the apnoea-hypopnoea index, the number of overnight respiratory events per hour of total sleep, the severity of obstructive sleep apnoea is classified as mild, moderate, or severe.15 Hence little of the polysomnographic data are used in clinical decision making because current practice is to largely reduce data complexity to a simple measurement (apnoea-hypopnoea index).16
As a standard of measurement, metrics aid in the differentiation of disease states and consequently classify the severity of the disease.40 A critique of the apnoea-hypopnoea index over the years has been its inability to accurately predict symptoms, treatment response, and the risk of long term health complications.40 41 This limitation might be partly because the apnoea-hypopnoea index does not capture the different physiological effects of respiratory events within and between individuals because all events are considered equal. Thus substantial interest has been reported in alternative metrics that can be extracted from polysomnograms that might reflect the severity of obstructive sleep apnoea and predict long term health complications better than the apnoea-hypopnoea index.42
New polysomnographic metrics, such as hypoxic burden, heart rate response to arousal, odds ratio product, quantitative EEG related metrics, and respiratory events load (eg, apnoea load), aim to use polysomnography to improve our understanding of sleep and sleep disorders43 44 (table 1). Specifically, hypoxic burden45 46 is calculated by assessing the area under the oximetry desaturation curve coupled with respiratory events. This metric seems to be better in predicting kidney disease,47 stroke,48 cardiovascular and cerebrovascular disease, and mortality than the apnoea-hypopnoea index in cohorts based in the clinic49 and in the community.21 We recognise, however, that there are other ways of measuring the degree of hypoxia in obstructive sleep apnoea. Because desaturation is a key feature of obstructive sleep apnoea and likely drives many of the end organ complications, further work to test these other types of metrics seems warranted.50 51
Polysomnographic metrics associated with outcomes of obstructive sleep apnoea
Another metric based on the physiological effects of obstructive sleep apnoea is heart rate response to respiratory events. Heart rate response to respiratory event was a better predictor of cardiovascular and cerebrovascular disease in patients with obstructive sleep apnoea.52 Also, a 2022 study showed that a greater heart rate response to respiratory events before treatment was associated with greater protection of continuous positive airway pressure against adverse cardiovascular outcomes.53
Indices derived from EEG signals based on polysomnography that better reflect the depth of sleep might also be useful to more accurately characterise patients. Based on a spectral analysis of EEG signals with fast Fourier transformation, relative frequency power in an array of frequency ranges (delta, alpha, theta, and beta) can be calculated.54 With proprietary scoring methods, these frequency powers can then be converted to a continuous measurement of sleep depth, the odds ratio product.55 Patterns of odds ratio product across the night could help to classify patients according to symptoms (eg, concomitant insomnia and obstructive sleep apnoea)56 and might help predict adherence to continuous positive airway pressure in severe obstructive sleep apnoea.57
Lechat and colleagues investigated the association between disrupted delta power (calculated by entropy and power spectral analysis of the EEG delta frequency band) and all cause mortality.58 They showed that disrupted delta power (upper and lower thirds of entropy function) during sleep was associated with a 32% increased risk of all cause mortality compared with no fragmentation (mid-third of the entropy distribution function) (hazard ratio 1.32, 95% confidence interval 1.14 to 1.50), after adjusting for confounders.
Finally, investigating how the severity of respiratory events would affect outcomes in patients with obstructive sleep apnoea showed that apnoea or hypopnoea load, which considers the length of the event and not only the presence or absence of events, was a better indicator of sleepiness than the apnoea-hypopnoea index alone.59 These new metrics could provide a more nuanced representation of the disease and help predict complications. These metrics need to be validated in other cohorts, however, before they can be used in medical decision making.42
Circulating biomarkers of risk
Biomarkers refer to a broad subcategory of medical signs.60 For this review, however, we will focus on recent data on circulating molecular markers of the risk of cardiovascular disease in obstructive sleep apnoea. Biomarkers are important assessable indicators that can provide complementary information for many diseases, including obstructive sleep apnoea,61 cardiovascular diseases,62 diabetes mellitus,63 hypertension,64 stroke,65 asthma,66 and heart failure.63
Intermittent hypoxia and consequent reoxygenation injury are a hallmark of obstructive sleep apnoea.61 67 Patients with obstructive sleep apnoea have increased circulating biomarkers of inflammation and oxidative stress (eg, adhesion molecules, C reactive protein, and 8-isoprostane).68–70 Therefore, biomarkers reflecting these processes of inflammation and oxidative stress could provide prognostic information on the risk of cardiovascular disease in obstructive sleep apnoea. Identifying a high risk group could have major clinical use because they might represent a target population for more aggressive management of obstructive sleep apnoea and other risk factors.71
In a recent study, multivariate protein measurement was used to quantify 5000 proteins cross sectionally in the plasma of 1391 clinic patients in relation to the presence and severity of obstructive sleep apnoea.72 The effect of treatment with continuous positive airway pressure or positive airway pressure on the proteins identified was also examined to explore potential pathophysiological mechanisms in two separate intervention based cohorts with obstructive sleep apnoea. The study showed that eight proteins (tissue type plasminogen activator, amyloid-like protein 1, plasminogen activator inhibitor 1, secretogranin 3, cystine-rich protein 1, prosurvival protein 1, sex hormone binding globulin, and desmoglein 2) likely predicted the presence and severity of obstructive sleep apnoea; and five protein markers (C reactive protein, tissue type plasminogen activator, plasminogen activator inhibitor 1, tartrate resistant acid phosphatase type 5, and soluble E-selectin) were significantly affected by continuous positive airway pressure or positive airway pressure (P=0.004, P=0.047, P=0.007, P=0.009, P=0.030, respectively).72 These results suggested that the subset of proteins might be promising markers in the management of obstructive sleep apnoea.
Markers of inflammation might also help group patients with obstructive sleep apnoea. In a pilot study of 155 patients with suspected obstructive sleep apnoea, increased levels of C reactive protein were associated with a markedly increased risk of cardiovascular and cerebrovascular disease. Specifically, patients with a C reactive protein concentration >2.38 mg/L had a significantly increased risk of cardiovascular and cerebrovascular disease within eight years of polysomnography (odds ratio 9.72, 95% confidence interval 2.43 to 38.84, P=0.001).73 Also, in a sample of 418 patients with suspected obstructive sleep apnoea, patients with higher levels of intercellular adhesion molecule 1 had a greater risk of cardiovascular events over eight years of follow-up, whereas patients with moderate-to-severe obstructive sleep apnoea with higher levels of E-selectin were more likely to have cardiovascular events.74 A genetic single nucleotide polymorphism that we previously found to be strongly associated with levels of E-selectin (ie, location rs579459 of the ABO gene) was also significantly associated with incident cardiovascular events (P=0.02),75 suggesting that genomic markers might also help with the prediction of risk.76 The limitations of these studies include the relatively small number of events and single centre design; clearly, more work is needed to replicate and expand these preliminary findings. Nevertheless, these results show the potential of inflammatory biomarkers to group potential of inflammatory biomarkers to help risk stratify patients by future cardiovascular risk.
Obstructive sleep apnoea is a common risk factor for hypertension, but in 25-30% of patients with obstructive sleep apnoea who were treated with continuous positive airway pressure (>4 hours/night), a positive effect on their blood pressure was not seen.77 The underlying mechanisms of this variability in response to continuous positive airway pressure are not known. MicroRNAs (miRNAs, a subclass of small single stranded non-coding RNAs) are important in regulating many biological processes and human diseases,78 including obstructive sleep apnoea.79 One study used an 84 miRNA array to discriminate plasma miRNA profiles and predict blood pressure responses to treatment with continuous positive airway pressure in patients with obstructive sleep apnoea and resistant hypertension.80 A cluster of three plasma miRNAs predicted patients with obstructive sleep apnoea with resistant hypertension, whose blood pressure adequately responded to treatment with continuous positive airway pressure. These results need to be replicated in larger cohorts to see if plasma miRNAs might eventually be clinically useful as biomarkers of cardiovascular risk.
A more precise molecular phenotyping of obstructive sleep apnoea with these and other markers could provide a more nuanced representation of the disease. Ultimately, this advanced phenotyping might provide more accurate care, matching precise subtypes to specific treatments. For example, patients with increased levels of biomarkers of oxidative stress or inflammation might have a more robust response to antioxidants or anti-inflammatory drugs, respectively, to reduce the risk of cardiovascular disease.81
Future research directions
Substantial work has been completed regarding personalised care approaches to obstructive sleep apnoea.12 However, substantial limitations to the current state of knowledge exist, and more work is needed before theses approaches can be implemented into clinical practice. Primarily, the use of subtypes of obstructive sleep apnoea defined by endotypes, polysomnographic markers, symptoms, and circulating biomarkers identified in previous studies need to be validated and confirmed in other cohorts that reflect a broader and more diverse patient population (eg, in terms of ethnic group,47 sex,82 and comorbidities83). The prevalence of obstructive sleep apnoea varies substantially by sex,84 and distinct differences exist between men and women in physiology, symptoms, and clinical outcomes of obstructive sleep apnoea.82 Many of the cohorts have included predominantly men, and more studies in women are needed to validate the potential measures discussed in this review. Differences among ethnic groups and other factors might exist; hence more studies that represent a more diverse patient group need to be completed before these measures can be implemented more broadly into clinical practice.
More work is needed to better integrate patients' perspectives and increase participation of patients and caregivers in their clinical care (ie, the participatory component of the P4 approach to personalised medicine).85 Also, because these personalised approaches will put a greater burden on patients (eg, collection of blood and urine samples), on analytical resources and platforms, and on financial costs, studies examining the economic return of this approach (eg, cost effectiveness studies) are also required before large scale investment. The gap between our current conceptual stage and accepted clinical practice is still wide.
Conclusions
Obstructive sleep apnoea is a heterogeneous disease, and a one-size-fits-all approach to the disease is likely not appropriate. In this review, we have highlighted potential future directions towards a better understanding of the heterogeneity of obstructive sleep apnoea and a precision care approach. Specifically, we have highlighted the emerging role of symptom clusters, physiological endotypes, advanced polysomnographic metrics, and circulating biomarkers in helping to group patients with obstructive sleep apnoea based on risk. We see a future paradigm of care where information from multiple sources is incorporated into statistical models to predict which patients have an increased risk of long term health complications, and to help match patients to more precise treatments (figure 1). This approach should provide a more nuanced representation of the disease for patients and providers, and help in moving research in this area forward.

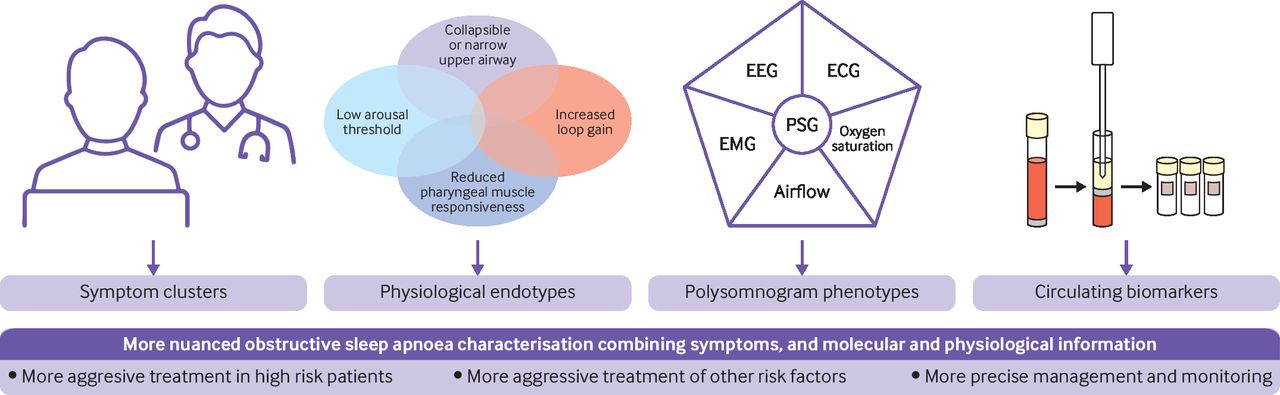{kind=link}
Precision care management for obstructive sleep apnoea with symptom clusters, polysomnogram phenotypes, physiological endotypes, and circulating biomarkers. PSG=polysomnography; EEG=electroencephalography; ECG=electrocardiography; EMG=electromyography
Questions for future research
How can we more precisely assess the underlying differences of patients with obstructive sleep apnoea by using clinical symptoms, physiological endotypes, advanced polysomnographic metrics, and circulating biomarkers?
How can we use more precise phenotyping of patients to help predict the long term effects on health of obstructive sleep apnoea, and match patients to the most appropriate treatment?
How can we accelerate the translation of research to help advance the treatment and diagnosis of obstructive sleep apnoea?
How can we begin to apply a personalised medicine approach to patients with obstructive sleep apnoea in the clinical setting?
Patient involvement
Patients and the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
References
Footnotes
Contributors All authors defined the intellectual content, conducted the literature research, acquired the data, and participated in the preparation, editing, and critical review of the manuscript. All authors have given final approval of the manuscript. NA is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests We have read and understood the BMJ policy on declaration of interests and declare the following interests: none.
Provenance and peer review Commissioned; externally peer reviewed.