Article Text

Abstract
Aim: To determine whether a combination of mood and personality factors together with illness beliefs and behaviours predict the onset of irritable bowel syndrome (IBS) post gastroenteritis, as suggested by the cognitive behavioural model of IBS.
Methods: Primary care patients with a positive test for Campylobacter gastroenteritis, and no previous history of IBS or serious bowel conditions were recruited into this prospective study (n = 620). Participants completed a questionnaire at the time of infection, which included standardised measures of mood, perceived stress, perfectionism, negative illness beliefs and illness behaviours. Participants completed follow-up questionnaires designed to determine whether they met the Rome criteria for IBS 3 and 6 months after initial infection.
Results: A total of 49 participants met the criteria for IBS at both follow-up points. Logistic regressions indicated that those who developed IBS had significantly higher levels of perceived stress (1.10, 95% CI 1.02 to–1.15), anxiety (1.14, 95% CI 1.05 to 1.23), somatisation (1.17, 95% CI 1.02 to 1.35) and negative illness beliefs (1.14, 95% CI 1.03 to 1.27) at the time of infection than those who did not develop IBS. Patients with IBS were also significantly more likely to remain active in the face of their acute symptoms until they felt forced to rest (all-or-nothing behaviour) (1.09, 95% CI 1.03 to 1.16), and significantly less likely to initially rest in response to their acute illness (0.93, 95% CI 0.88 to 0.97). Depression and perfectionism were not associated with the onset of IBS.
Conclusions: Results suggest that patients with high stress and anxiety levels are more prone to develop IBS after a bout of gastroenteritis. Additional risk factors include a tendency to interpret illness in a pessimistic fashion and to respond to symptoms in an all-or-nothing manner.
- BRIQ, Behavioural Responses to Illness Questionnaire
- IBS, irritable bowel syndrome
- PCA, principal component analysis
Statistics from Altmetric.com
- BRIQ, Behavioural Responses to Illness Questionnaire
- IBS, irritable bowel syndrome
- PCA, principal component analysis
Irritable bowel syndrome (IBS) is a chronic condition characterised by abdominal pain and associated bowel disturbance. IBS affects as many as 10–15% of the adult population in Western countries, but the condition remains poorly understood.1 No single cause adequately explains the symptoms and, in the absence of clear structural pathology, an aetiological debate has been polarised in a mind/body split.2–5 More recently, it has been acknowledged that models capable of integrating biological and psychological domains are necessary to explain the heterogeneity associated with the condition.6–9
One of these models, based on cognitive behavioural theory,10 has been developed to explain a range of functional somatic syndromes including IBS.11,12 This model suggests that people at risk of IBS have anxious or depressive tendencies with high, and often unrealistic, personal expectations (high levels of perfectionism). When such individuals experience an infection such as gastroenteritis, their need to perform suggests that their initial reaction may be to press on and remain active. However, this ultimately worsens symptoms, forcing them to rest for a period. Resting conflicts with the perfectionist’s desire to achieve, and heightens feelings of anxiety and stress. As a result, they very quickly try to return to premorbid levels of activity. Stress and overactivity ultimately exacerbate symptoms again and they return to bed. This pattern of pushing too hard or being overactive and then needing to rest for prolonged periods is known as all-or-nothing behaviour. If this behaviour is repetitive, patients may start to believe that they have a chronic incurable condition, and become increasingly distressed by their ongoing symptoms and illness. Distress in turn helps to maintain the symptoms.
There is some evidence for the risk factors outlined in this model. In support of biological infections, a number of studies have shown that various forms of gastroenteritis are risk factors for the development of IBS.13–15 Psychology also plays a role. Sykes et al16 showed that people with premorbid psychiatric diagnoses, particularly anxiety disorders, were at greater risk of developing IBS after gastroenteritis. Similarly, depression, neuroticism, somatisation and stress have all been linked to the onset of IBS.17,18 Finally, Parry et al19 found that patients with gastroenteritis who had more negative perceptions of their infection were more likely to develop IBS.
A limitation of these studies is that they investigate either individual risk factors or a limited number of risk factors. None of the prospective investigations appear to have used a model to guide their choice of variables. The purpose of the current study was to provide a more complete evaluation of the cognitive–behavioural model as it applies to IBS. Specifically, we aimed to study an at-risk cohort with gastroenteritis in order to determine whether the key psychological risk factors in the model would interact with the infection in predicting the onset of IBS 6 months after infection. We were interested in looking at the contribution of each variable individually, as well as at the relative risks posed by the different factors.
SUBJECTS AND METHODS
Design and procedure
This study used a prospective cohort design. Patients with a confirmed diagnosis of Campylobacter gastroenteritis were invited to participate in the study at the time of their acute illness. They completed a baseline questionnaire which included a range of potential risk factors for IBS at the time, or close to the time, of their acute illness. Follow-up questionnaires to determine the new incidence of IBS were completed 3 and 6 months later.
Potential participants were recruited from the largest provider of community clinical diagnostic services in Auckland, using consecutive sampling over a 10-month period. Individuals over the age of 16 years with a positive test result for Campylobacter gastroenteritis were eligible to participate in the study.
Positive tests were determined by isolating Campylobacter species from stool samples which were inoculated onto charcoal–cefoperazone–deoxycholate agar and incubated in a microaerophilic atmosphere for 72 h. Suspect colonies that were oxidase positive and revealed Gram-negative curved bacilli after gram staining were reported as Campylobacter species.
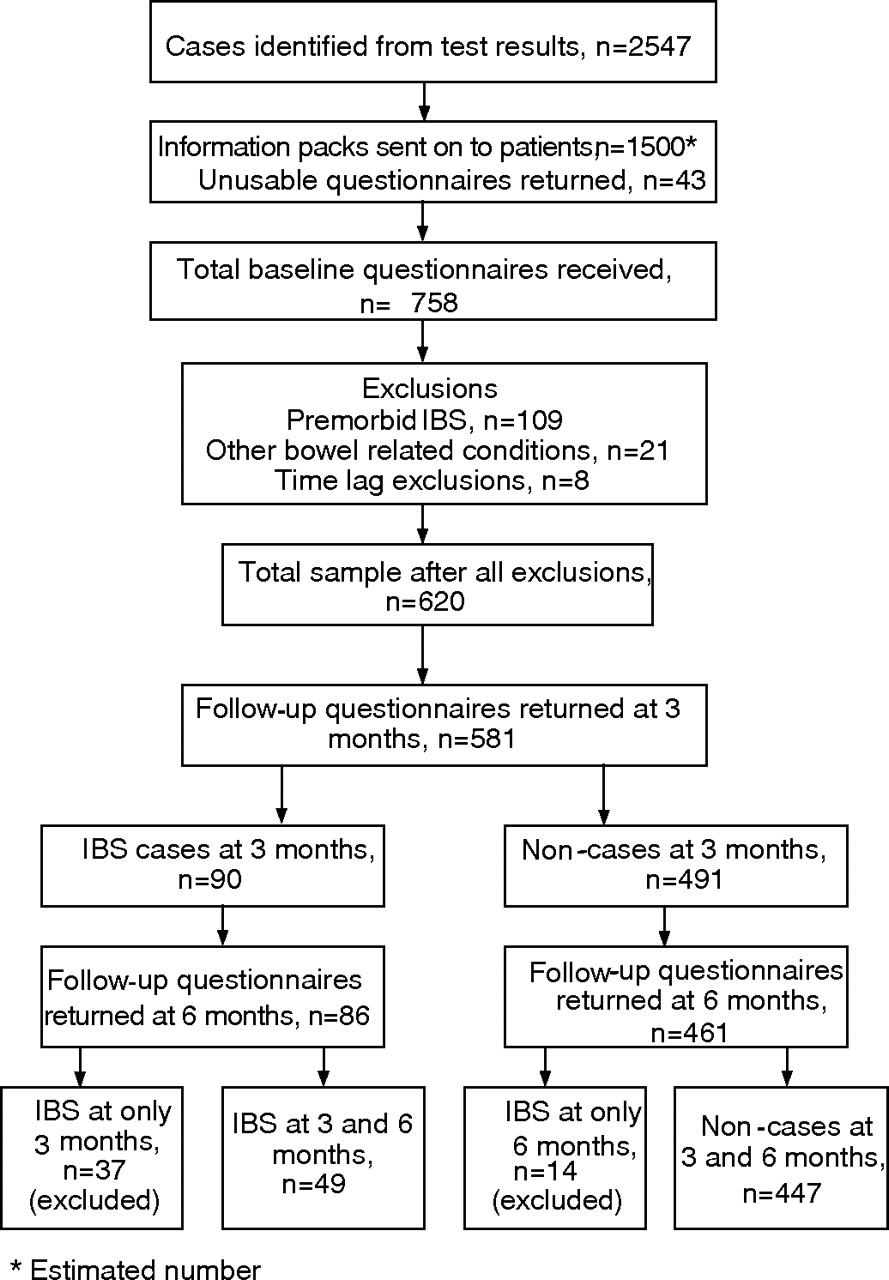
Patients were unable to be contacted directly due to the confidentiality of health information, so for each identified case (n = 2547) the laboratory sent a pack including an information sheet, consent form and questionnaire to the individual’s general practitioner to be forwarded on. Follow-up of the general practices indicated that around 60% of general practitioners forwarded information about the study to their patients, suggesting that approximately 1500 questionnaires reached potential participants. A total of 801 questionnaires were returned; however, 36 had not reached the intended participant due to incorrect addressing, and 7 completed questionnaires were returned without consent forms. The total remaining usable questionnaires numbered 758; a response rate of 52% consistent with the rate found in another large community survey.20 Figure 1 illustrates the flow of participants.

{kind=link}
Flow of participants through the study. IBS, irritable bowel syndrome.
We based our power analysis on a study using similar recruitment and diagnostic methods as ours, which found a post Campylobacter prevalence rate of 17% for IBS.14 Using 80% power and a 0.05 level of significance, a sample of 585 Campylobacter cases was needed to detect a true difference in the proportions becoming an IBS case.
The Auckland Ethics Committee approved this study (2001/303) on 18 January 2002.
MEASURES
Baseline questionnaire
The baseline questionnaire included questions about demographics, illness symptoms and treatment, history of IBS and bowel-related disorders, and a number of psychological measures described below.
The number of Campylobacter symptoms experienced was summed to provide an indicator of illness severity. Patients completed a checklist of symptoms including nausea, headache, fever, vomiting, diarrhoea, stomach pain, blood in faeces and aching muscles.
The remaining baseline questionnaires were included to operationalise the psychological variables described in the cognitive–behavioural model of IBS. The Hospital Anxiety and Depression Scale21 was used to assess the severity of anxiety and depression experienced in the month before infection. The symptom checklist described above also included a number of non-specific symptoms taken from the illness identity scale of the Illness Perceptions Questionnaire-Revised.22 Manifestations of symptoms such as sore eyes, loss of strength, feeling off colour, breathlessness, joint pain, dizziness, unrefreshing sleep, racing heartbeat and feeling worse after exertion were totalled as a measure of general somatisation.
The negative subscale from the Positive and Negative Perfectionism Scale23 was included as a measure of perfectionism. Several studies have found the negative rather than the positive subscale to have the strongest predictive validity across a variety of conditions.24–26 The 10-item Perceived Stress Scale27 was used to assess participants’ perceptions of their levels of stress in the month prior to infection.
The Illness Perception Questionnaire-Revised22 was included to measure the degree to which patients viewed their acute illness in a negative manner. The questionnaire was modified to reduce the overall size of the scale and to make it more relevant to patients with gastroenteritis. Subscales measuring beliefs about how long they thought the illness would last, how serious they believed the consequences of the illness to be, and how emotionally distressed and puzzled they were by their illness were combined to form a negative illness beliefs score for each individual. Finally, the all-or-nothing and limiting behaviour subscales from the Behavioural Responses to Illness Questionnaire (BRIQ)28 were used in order to determine the effect of specific behavioural responses at the time of acute illness. The limiting scale measures the extent to which patients rest and reduce activity in response to illness, and includes items such as “I have avoided my usual activities” and “I have gone to bed during the day”. The “all-or-nothing” scale measures a pattern of overactivity and then rest, and includes items such as “I have overdone things, then needed to rest up for a while” and “I have pushed myself as hard as ever until I cannot push myself any more”.
Follow-up questionnaire
Participants were sent a follow-up questionnaire designed to identify participants who met the diagnostic criteria for IBS 3 and 6 months after the date of their stool sample. Table 1 summarises the criteria used for diagnosing IBS. Rome I cases were determined by using the modified option that requires both pain-related symptoms and the disturbed-defecation criteria.29 Individuals were classified as meeting Rome I criteria if they reported one or more abdominal pain-related symptoms and two or more symptoms of disturbed defecation at least 25% of the time (see table 1 for details of symptoms). Rome II cases were determined on the basis of the presence of two or more abdominal pain-related symptoms present for ⩾3 months.30 In recent years, there has been an ongoing debate as to the usefulness of the distinctions made by these criteria.31–33 Because of this debate, and in order to gain the most representative group of IBS cases, it was decided to determine as one category those participants who met either Rome I modified or Rome II criteria as cases of IBS at both time points.
Self-report information used to determine caseness groupings for irritable bowel syndrome
Statistical analysis
All analyses were conducted on SPSS V.12.1. Demographic, illness and mood variables were compared between the IBS cases and non-cases using independent-sample t tests and χ2 tests. The significance of each individual psychological variable as a risk factor for the development of IBS was examined using binary logistic regression analyses. IBS outcome was entered as the dependent variable (coded 0 for “no IBS” and 1 for “IBS”) with each psychological variable measured at baseline entered into separate regression analyses as a covariate with gender, age, Campylobacter symptoms and antibiotic prescription to ensure that any significant effects were independent of these potentially confounding variables.
In order to determine the relative importance of the psychological variables, the eight predictor variables were reduced to a smaller number of factors using principal component analysis (PCA) with varimax rotation. Reducing the number of predictor variables was necessary, as many of these variables were intercorrelated which creates the problem of multicollinearity. These factor scores were then entered into a single logistic regression analysis, controlling for possible confounds as above and with IBS outcome as the dependent variable.
RESULTS
Response rates, exclusions and demographics
A total of 90 (15%) new cases of IBS who met the criteria at 3-month follow-up and 63 (12%) who met the criteria at 6-month follow-up were identified. Because Rome III criteria for IBS,34 published subsequent to this study, specify that patients must have experienced symptoms for 6 months and not for 3 months as in Rome I and II, data were analysed using only cases of those who met the criteria at both time points. To avoid confounding the findings, participants who met criteria for IBS at one of the time points only were excluded from the analyses. This included 37 participants who met the criteria at 3 months only and 14 who met the criteria at 6 months only (total n = 51). Consequently, data were analysed for 447 non-cases and 49 (10%) cases of IBS (see fig 1 for details of inclusions and exclusions).
Table 2 compares cases and non-cases on demographic, mood and illness variables. The IBS cases were significantly more likely to be female than non-cases (Pearson χ2 (1, n = 496) = 10.47, p⩽0.001), whereas the non-cases were significantly older than IBS cases (t (492) = 2.3, p = 0.03). With regard to illness variables, there was no difference in the number of reported Campylobacter specific symptoms at the time of acute illness between the two groups (t (494) = –1.6, p<0.12), nor did they differ in the rate of prescription of antibiotics (Pearson χ2 (1, n = 488) = 0.23, p = 0.63). IBS cases were significantly more anxious (t (492) = –3.98, p<0.001) and stressed (t (492) = –4.29, p<0.001) at the time of infection than non-cases, but there was no difference between the groups in levels of depression (t (492) = –0.95, p = 0.34).
Comparison of post-Campylobacter irritable bowel syndrome cases and non-cases on demographic, illness and mood variables
Significance of the psychological variables
Table 3 presents the results from the logistic regressions which looked at each psychological predictor individually. For the sake of simplicity, the statistics for the effects of gender, age, Campylobacter symptoms and antibiotic prescription are not presented. These can be summarised as follows: age, number of Campylobacter symptoms and antibiotic prescription were not significant risk factors for the development of IBS in any of the eight individual analyses, whereas gender was a significant risk factor in all analyses.
Individual logistic regression analyses of irritable bowel syndrome outcome post-Campylobacter as a function of individual psychological variables
Six of the eight psychological variables were predictors of IBS caseness, the exceptions being depression and perfectionism. In accordance with the model, IBS cases reported significantly higher levels of anxiety, somatisation, perceived stress, negative illness beliefs and all-or-nothing behaviour at the time of the acute infection. IBS cases were also significantly less likely to have limited their activity levels in response to their gastroenteritis.
Relative importance of the psychological variables
The number of psychological variables was reduced using PCA. The first PCA produced three factors with eigen values >1; however, examination of the screen plot suggested that a four-factor solution may be more appropriate. A four-factor solution was imposed and results of this PCA indicated that these four easily interpretable factors explained 75% of the variance, with all variables producing factor loadings >0.66. The factors were labelled anxious achievement, negative beliefs, illness behaviour and all-or-nothing behaviour (table 4). The subscales making up each factor loaded no more than 0.46 on any other factor, with most obtaining loadings of <0.20.
Principal components analysis of the psychological variables
The four factor scores were entered as covariates along with gender, age, antibiotic prescription and Campylobacter symptoms into a regression equation, with IBS outcome as the dependent variable. Table 5 presents the results, and indicates that the anxious-achievement factor and all-or-nothing behaviour were both significant risk factors for the development of IBS, with those reporting higher levels of these variables at the time of acute illness more likely to develop IBS. Gender was also a significant risk factor, with women having 2.6 times the odds of developing IBS post-gastroenteritis than men.
Logistic regression analyses of irritable bowel syndrome outcome post-Campylobacter as a function of gender, Campylobacter symptoms, age, antibiotic use and psychological factor scores
DISCUSSION
This study is the first to prospectively investigate a combination of emotional, cognitive and behavioural risk factors relevant for the development of IBS after Campylobacter gastroenteritis. The results generally supported the cognitive–behavioural model, with higher levels of anxiety, somatisation, perceived stress and negative illness beliefs all found to be significant risk factors for the development of IBS 6 months after infection. Patients with IBS were also more likely to have reported a tendency to be overactive in the face of their symptoms until they could no longer carry on (all-or-nothing behaviour), and less likely to initially rest or reduce activity in response to their acute illness (limiting behaviour). Depression and perfectionism were not significant risk factors in the development of IBS.
When considering the relative importance of these variables, multivariate analysis of four factors identified using principal components analysis found that an anxious-achievement cluster of variables (made up of anxiety, stress and perfectionism) and an all-or-nothing behaviour on its own were the most important predictors of IBS along with female gender. These results support the hypothesis that the predisposition to IBS may be mediated by unrealistic personal expectations in the context of high levels of perceived stress and anxiety. These predispositions lead patients to respond to illness by initially not allowing themselves time to recover, which ultimately leads to an all-or-nothing pattern of responses.
These results are largely in keeping with past studies, although there are some differences—for example, the importance of negative illness beliefs is in accordance with previous studies in this area19 as is the significance of anxiety and somatisation.17,35 Depression, however, was not significantly associated with IBS, in contrast with earlier studies.17,35 This discrepancy may be the result of the different sampling strategies utilised within these studies: the Gwee Study used patients hospitalised with gastroenteritis, whereas the Dunlop Study carried out physical examination and testing procedures and recruited only 30 of 103 new-onset IBS cases identified, perhaps reflecting those more distressed about their condition.
Stress has also been considered an important precipitant in the cognitive behavioural model of IBS; however, the empirical evidence from retrospective and cross-sectional studies has been inconsistent.36 One other prospective study of post-infectious IBS found that higher levels of life events in the 12 months prior to gastroenteritis were associated with the development of IBS.18 The current study has further clarified the role of stress with the finding that levels of perceived stress are also strongly associated with the development of IBS, indicating that the individual’s interpretation of stressful events may be as important as the nature of those events.
Negative perfectionism is also hypothesised to be a risk factor in the cognitive–behavioural model of IBS, but has not previously been studied prospectively. This study provides some indication that although on its own it may not be a risk factor for IBS, in combination with anxiety and perceived stress it becomes more relevant. It is possible that the predisposition to IBS may be mediated by unrealistic personal expectations in the context of high levels of perceived stress and anxiety.
The investigation of behavioural factors in the development of IBS has previously been neglected. In contrast with previous studies that have considered bed rest at the time of acute illness as a potential barrier to recovery,37,38 such limiting behaviour was actually protective in this study. Instead, the most important behavioural risk factor appeared to be the oscillating pattern—that is, bursts of activity in conjunction with periods of rest.
The current results relate to behaviour at the time of acute illness, but it is also possible that these behaviours, along with negative illness beliefs, represent patterns that endure over time. Individuals with an all-or-nothing response to acute illness may have a similar approach to IBS symptoms, and therefore may be at greater risk of perpetuating those symptoms. In order to clarify the role of illness beliefs and behaviour in the perpetuation of IBS, the findings from the current study need to be replicated in longitudinal studies of patients with IBS.
We also investigated other variables relevant to the development of IBS, including gender, the extent of gastroenteritis symptoms and the use of antibiotics. Gender was a significant predictor in all analyses undertaken, with females twice as likely to go on to develop IBS as males. This result is consistent with previous primary care and community studies.39 The fact that females are at greater risk for the illness warrants further attention. A higher Campylobacter symptom total and the prescription of an antibiotic were not found to be significantly associated with IBS following Campylobacter. Although these measures do not provide an objective measure of clinical severity, these results do contrast with findings from previous studies indicating that acute illness severity is a risk factor for the development of post-infectious IBS.40,41 Future work in this area should include the investigation of the ongoing post-infectious inflammatory processes in the bowel and their inter-relationships with the psychological variables in predicting IBS onset.
When interpreting the findings of this study, certain limitations need to be taken into account. Although we had excellent follow-up rates, the initial response rate in the study was low. We have tested the model only in one at-risk sample. Not all cases of IBS will have experienced a prior infection, and individuals with a post-infectious onset belong to a specific subset of cases.42 Future prospective studies using other at-risk samples (such as victims of psychological trauma or patients undergoing surgery) may help to clarify the role of the cognitive–behavioural variables.
It is also possible that the behaviours and cognitions included in this study were measured at a time when those with the most severe Campylobacter were still ill whereas those with more mild symptoms had recovered. In an attempt to control for this, we included the number of symptoms and antibiotic use as covariates in the analyses presented. We were unable to use length of symptoms as a covariate as many of the patients completed the questionnaires when they were still experiencing symptoms.
Our sample also relied on patients who received diagnostic confirmation of their infection. Only a small minority of patients consult a doctor with gastroenteritis, so patients who get tested for the bacteria are not necessarily representative.43 Future studies of outbreaks of gastroenteritis such as that conducted by Ji et al44 represent a way around this problem, and are needed to replicate these results.
Finally, we used postal questionnaires to determine IBS caseness. Although there is evidence to suggest that it is possible to identify IBS using self-report questionnaires,45 there is a risk that a number of participants would be wrongly included in the study—that is, would be classified as having the condition when in fact they do not (and vice versa). Several procedures were included in the study to reduce the likelihood of this; published diagnostic criteria were used to determine IBS caseness at follow-up, and the exclusion criteria were conservative so as to reduce the number of false positives. The resulting prevalence rates reported in the Results section are comparable with those found in previous studies,14,18,46 indicating that these procedures had the desired effect.
Despite these limitations, the current study provides support for the cognitive–behavioural model of IBS. The results add to our earlier study which showed that Campylobacter gastroenteritis was a stronger predictor of IBS than glandular fever.43 The current study suggests that this biological event may interact with a range of psychological variables in causing the onset of IBS. Gastroenteritis may trigger the symptoms, but cognitions, behaviour and emotions may help to prolong and maintain them over time. This provides support for cognitive–behavioural therapy as a treatment for IBS. It also suggests that patients who have ongoing symptoms following gastroenteritis may benefit from a simple early cognitive–behavioural intervention where they are encouraged to slowly regain levels of activity and to avoid fluctuating between overactivity and underactivity. Future research should focus on how these risk factors lead to symptoms in IBS so that we can get a better understanding of the interaction between biological and psychological factors.
Acknowledgments
This research was supported by a grant awarded to RM-M from the University of Auckland Vice Chancellor’s development fund and two scholarships awarded to MJS: a University of Auckland Doctoral Scholarship and a Foundation for Research, Science and Technology Scholarship. Our work was independent of these funding providers. We thank Dr Susan Taylor from Diagnostic Medlab for her advice and information on the diagnostic test used in this study, and for her invaluable help with recruitment. We also thank Grant Sutcliffe for designing and developing the Mailout tracker database for this study.
REFERENCES
Footnotes
-
Published Online First 26 February 2007
-
Competing interests: None.