Article Text

Abstract
Objective To examine the association of gout with cardiovascular outcomes using linked administrative health data in Aotearoa New Zealand.
Design Data linkage study.
Setting National registries of pharmaceutical dispensing, hospital admission, and deaths linked to the Auckland/Northland regional repository of laboratory results to create a regional health contact population as of 31 December 2011.
Participants 942 416 residents of the Auckland/Northland region, aged 20-79 years with no history of cardiovascular disease.
Main outcome measures Time to first fatal or non-fatal cardiovascular event, identified from national datasets on hospital admissions and mortality, between 1 January 2012 and 31 December 2016. Cardiovascular disease was broadly defined as comprising ischaemic heart disease, ischaemic or haemorrhagic stroke, transient ischaemic attack, peripheral vascular disease, and heart failure.
Interventions A history of gout identified from a discharge diagnosis of gout from a public hospital admission or previous dispensing of gout specific drug treatments. The cohort was then linked to national hospital admissions and deaths through to 31 December 2016 (ie, 5 years' follow-up). Multivariable Cox proportional hazard models were constructed to assess the associations between gout, other risk factors, and cardiovascular outcomes.
Results Of 942 416 people included in the study, 31 907 (3.4%) had gout (6261 women and 25 646 men). After adjustment for multiple risk factors for cardiovascular disease, gout was associated with increased cardiovascular events (adjusted hazard ratio 1.34 (95% confidence interval 1.23 to 1.45) in women; 1.18 (1.12 to 1.24) in men). For men with gout, there was an increased risk of cardiovascular disease in those who were not dispensed regular allopurinol (1.15 (1.05 to 1.25)) and those with a serum urate above the treatment target of 0.36 mmol/L (1.16 (1.04 to 1.30)). Risk of cardiovascular events was lower for men with gout who were not dispensed colchicine compared with those who were (0.84 (0.77 to 0.92)). These findings were not observed in women.
Conclusion These results indicate that gout is associated with an increased risk of cardiovascular events. In men with gout without history of cardiovascular disease, the cardiovascular risk was lower in those regularly dispensed allopurinol and those with serum urate levels at the recommended treatment target. By contrast, colchicine dispensing was associated with an increased risk of cardiovascular events in men with gout without a cardiovascular history. The potential causal mechanisms of these associations require further exploration, including casual inference modelling in future studies.
- Rheumatology
- Cardiology
- Epidemiology
Data availability statement
Data are available upon reasonable request. All individual participant (deidentified) data, including a data dictionary defining each field, will be made available to university based academic researchers if their proposed analyses are approved by the investigators’ data access proposal committee. A proposal must be considered relevant to the original aims of the research, must meet the study's ethics approval criteria, and will require one or more of the study investigators as formal collaborators. A signed data access agreement will be required and the costs of preparing the datasets will need to be covered. There are no set dates for when these data will be made available. Please contact the corresponding author regarding data sharing requests.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known about this topic
Evidence in the literature to support gout and hyperuricaemia as risk factors for cardiovascular disease is mixed
In a systematic review and meta-analysis of 32 studies, findings suggested a positive dose-response association between hyperuricaemia and cardiovascular mortality
Colchicine, a drug treatment primarily used in the management of gout, has been shown to reduce risk of future cardiovascular events in people with a history of cardiovascular disease
What this study adds
In this large nationally representative cohort from Aotearoa New Zealand, findings indicated an increased risk of cardiovascular events in people with gout, even after adjustment for other cardiovascular risk factors
Among men with gout without a history of cardiovascular disease, regular allopurinol dispensing and serum urate at treatment targets levels was associated with a lower risk of cardiovascular disease; however, colchicine dispensing was associated with an increased risk of cardiovascular events
How this study might affect research, practice, or policy
In people with gout and no history of cardiovascular disease, regular allopurinol dispensing and serum urate at treatment target levels could have an additional cardiovascular benefit beyond treatment of joint disease
Any potential causal mechanisms of these associations require further exploration including casual inference modelling in future studies
Risk of cardiovascular disease remains highest among Māori and Pacific Island people, with or without the additive risk factor of gout, highlighting the importance of resolving inequities in these population groups through access to timely and culturally safe care
Introduction
Some studies have reported that gout and hyperuricaemia are risk factors for cardiovascular events.1–5 However, other studies have not shown an association between hyperuricaemia and cardiovascular events after adjustment for established risk factors.6–9 In Aotearoa New Zealand, gout is the most common form of inflammatory arthritis, affecting over 4% of adults.10 Māori (indigenous New Zealanders) and Pacific Island people are disproportionately affected by gout, with the highest prevalence of the disease worldwide; gout affects about 9% of Māori adults and 14% of Pacific Island adults, and more than a third of Māori and Pacific Island adults older than 65 years living in Aotearoa New Zealand.10
While the benefit of the urate lowering drug allopurinol for the management of gout is well established,11–13 some evidence suggests a potential additional benefit of allopurinol on risk of cardiovascular disease. A cohort study of the US Multi-Payer Claims Database found that in people with gout and diabetes, current allopurinol users had a lower risk of incident stroke or myocardial infarction than previous allopurinol users (hazard ratio 0.67 (0.53 to 0.84)).14 This association persisted after adjustment for other risk factors for cardiovascular diseases, immune diseases, and colchicine use. Primarily used in the past for the treatment and prevention of gout flares, colchicine has also become of high interest for cardiovascular research. Two recent randomised controlled trials in people with a history of cardiovascular disease found that 0.5 mg daily use of colchicine confers a significant reduction in the risk of future cardiovascular events.15 16
Recently, risk equations used for the primary prevention of cardiovascular disease have been developed and validated solely using predictors available from routinely collected national health data in Aotearoa New Zealand (sex; age; ethnic origin; level of socioeconomic deprivation; diabetes status; previous admission to hospital for atrial fibrillation; and dispensing at baseline of blood pressure lowering, lipid lowering, or antiplatelet or anticoagulant drug treatments).17 While some clinical predictors (smoking, blood pressure, lipid levels) are not available in administrative health data, the predictors included in these equations enable individual level, cardiovascular risk to be examined across an entire population. We linked national and regional health databases in Aotearoa New Zealand and used these available predictors to investigate the association of gout with cardiovasculr outcomes. We then examined the effect of regular allopurinol dispensing, serum urate levels, and colchicine dispensing on cardiovascular risk in this population.
Methods
Source data and participants
Aotearoa New Zealand residents aged 20-79 years who were in contact with publicly funded health services in 2011, were still alive on 31 December 2011 and lived in the Auckland/Northland region were identified through anonymised, individual level linkage of national and regional health databases. National databases included hospital admissions, mortality, outpatient visits, primary care enrolment, primary care reimbursement (to capture primary care visits by non-enrolled patients), and community pharmaceutical dispensing. These databases were linked to the Auckland/Northland regional repository of all public, private, hospital, and community laboratory results, because no national repository of laboratory results currently exists. About a third of all New Zealanders live in this region, which includes Aotearoa New Zealand’s largest city (Auckland) as well as several towns and rural areas. The study data were anonymised by the encryption of the National Health Index (NHI) number that is assigned to every person who uses the publicly funded health system and uniquely identifies over 95% of the population.
We subsequently excluded individuals if they had been admitted to hospital previously for cardiovascular disease or heart failure between 1 January 1988 and 31 December 2011; had been dispensed loop diuretics or metolozone on at least one occasion as recorded in the national dispensing data between 1 July 2006 and 31 December 2011 to capture individuals who had heart failure but had not been admitted to hospital for it; had a primary residence outside of the Auckland/Northland region for the past three years; and had missing predictor data required to estimate cardiovascular risk (0.06% of the total eligible cohort). Further details regarding the first two criteria are provided in online supplemental appendix 1.
Supplemental material
We used a validated national health data definition of gout to identify participants with gout: a discharge diagnosis of gout (ICD-9 (international classification of diseases, 9th revision) code 274, ICD-10-AM (Australian modification) code M10) from a public hospital admission between 1 January 1988 and 31 December 2011 or dispensed drug treatments for gout (allopurinol or colchicine) between 2007 and 2011.10 For individuals who had been diagnosed with leukaemia or lymphoma (ICD-10-AM C80-C96), dispensing of allopurinol was excluded as an indicator of gout. In Aotearoa New Zealand, allopurinol is not recommended for the treatment of asymptomatic hyperuricaemia. Benzbromarone was not funded in Aotearoa New Zealand until April 2013 and febuxostat was not funded until July 2014. We did not include probenecid use in the definition because it is not used frequently in Aotearoa New Zealand for gout treatment and is often used to increase antibiotic blood levels for the treatment of bacterial infections in primary care.
Serum urate values were identified from the Auckland/Northland regional repository of laboratory results. In participants with multiple serum urate values, the value closest to the index date of 1 January 2012 was selected to most accurately reflect serum urate levels prior to enrolment. Based on recommendations for target serum urate for management of gout and as a surrogate for people with treated or untreated gout, we further categorised serum urate into those with a level below or greater than or equal to 0.36 mmol/L (6 mg/dL).18
Outcome
The outcome of interest was time to first fatal or non-fatal cardiovascular event, identified from national datasets on hospital admissions and mortality, between 1 January 2012 and 31 December 2016. A broad definition of cardiovascular disease was used, comprising ischaemic heart disease, ischaemic or haemorrhagic stroke, transient ischaemic attack, peripheral vascular disease, and heart failure, defined from ICD-10-AM codes.
Predictors of cardiovascular disease
The predictors for inclusion in the multivariable models (described below) were based on previously validated, sex specific prediction equations for the risk of cardiovascular disease. These equations are derived from national administrative health data,17 which allow the estimation of risk of a fatal or non-fatal cardiovascular event occurring over the following five years. Included predictors were age, ethnic origin, level of socioeconomic deprivation, diabetes status, previous admission to hospital for atrial fibrillation, and dispensing at baseline of blood-pressure lowering, lipid lowering, or antiplatelet or anticoagulant drug treatments at least once in the six months before 1 January 2012.
Ethnic origin was categorised according to categories recorded in the NHI dataset, which is based on the Ministry of Health’s Ethnicity Data Protocols for the Health and Disability Sector. For individuals with more than one ethnic group recorded in the NHI dataset, a single ethnic group was assigned using the following prioritisation order: Māori, Pacific Island people, Indian, Chinese, other, New Zealand European. In Aotearoa New Zealand, ethnic origin recording in health data currently enables identification of Indians (who comprise about 90% of South Asians in Aotearoa New Zealand) but not other South Asian groups such as Pakistanis. People who were not in the most common categories for ethnic origin were grouped into the "other" category, including non-Chinese Asian, non-Indian Asian, Middle Eastern, Latin American, African, and unspecified. Socioeconomic deprivation was determined from the New Zealand Index of Deprivation (NZDep, 2006),19 which is a small, area based measure assigned to people living in a defined geographical area (mesh block). NZDep is based on nine variables from the national census—income, employment, access to car or telephone, household living space, educational qualifications, and social support. For these analyses, NZDep was grouped by quintiles into five groups, with group 1 being the least deprived and group 5 being the most deprived.
Statistical analysis
We used multivariable Cox proportional hazards regression using time from 1 January 2012 as the time scale to compare the risk of total cardiovascular events over five years in women and men with and without gout. Models for women and men were constructed to assess predictors included in the sex specific equations as well as the addition of gout (yes/no) (model 1), regular dispensing of allopurinol (model 2), serum urate level (model 3) and dispensing of colchicine (model 4). These models included adjustment for age; ethnic origin; level of socioeconomic deprivation; diabetes status; previous admisstion to hospital for atrial fibrillation; and dispensing at baseline of blood pressure lowering, lipid lowering, or antiplatelet or anticoagulant drug treatments at least once in the six months before 1 January 2012.
For model 2, we defined regular dispensing as allopurinol dispensed from a community pharmacy in at least three of four quarters of 2012. For model 3, serum urate levels in indivdiuals with gout was categorised by recent concentrations of <0.36 mmol/L or ≥0.36 mmol/L, or in those did not have serum urate testing in the previous three years. For model 4, colchicine dispensing for individuals with gout were categorised by those who were dispensed colchicine at least once in the previous 12 months compared with those who were not dispensed colchicine. Given the ethnic differences in gout prevalence,10 the interaction between gout and ethnic origin was examined for model 1. Unlike in model 1, where the reference group was people without gout, the reference groups in models 2-4 changed to the preferred or typical scenario for people with gout (model 2, people with gout who were dispensed allopurinol in three of four quarters of 2012; model 3, people with gout who had a recent serum urate level of <0.36 mmol/L; model 4, people with gout who were dispensed colchicine in the previous 12 months). These reference groups were selected to investigate the potential associations between urate lowering treatment, colchicine, and cardiovascular disease.
Validity of the proportional hazards assumption was assessed through visual inspection of scaled Schoenfeld residual plots and a score test that the slope of residuals over time is zero. Only age group among men might have had a non-proportional hazard—the relation over time was consistent across models, and on balance, we decided to continue because the factor's inclusion would not materially affect the findings of this study. All variables were categorical, including age, and follow-up was censored when a non-cardiovascular death occurred. We have previously undertaken competing risk analyses using this cohort and found it was unnecessary owing to the short follow-up. We used R statistical software version 3.6.0 (2019-04-26) for all analyses.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Study cohort characteristics
In 2011, 1 040 832 Auckland and Northland adult residents were in contact with publicly funded health services and alive as of 31 December 2011. At the inception date of 1 January 2012 and after exclusions for age (n=43 971), previous cardiovascular disease (n=53 608), or missing predictor data (n=837), 942 416 people remained in our study cohort—31 907 people with gout and 910 509 people without gout (figure 1).
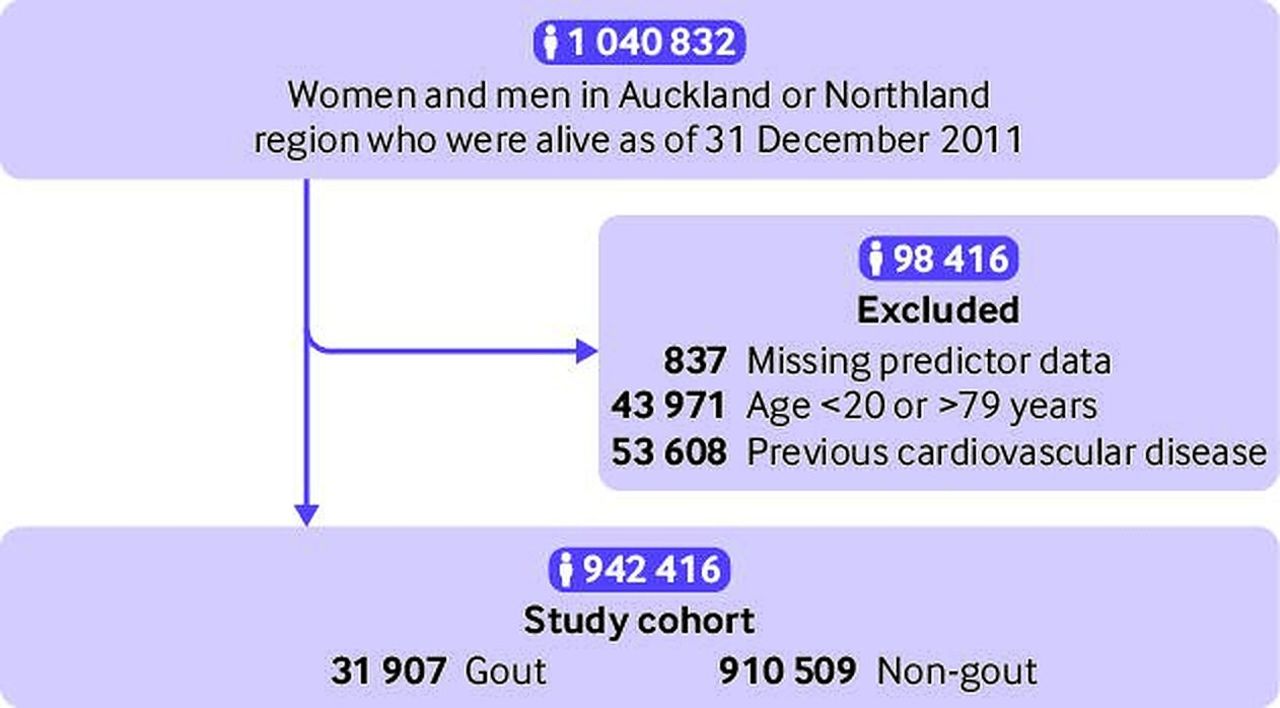
Exclusions and formation of study cohorts (2012-16)
Baseline characteristics are presented in table 1. People with gout were older than people without gout, more likely to be men (80% with gout v 44% without gout), and more likely to reside in the two most socioeconomically deprived groups than people without gout. The gout cohort had a higher representation of Māori and Pacific Island ethnic groups (50% of women and 44% of men) than the non-gout cohort (22% and 19%, respectively); and the prevalence of gout was highest among Māori and Pacific people (9% of Māori men, 2% of Māori women; 16% of Pacific Island men, 3.5% of Pacific Island women). Only 37% of women and 41% of men with gout had allopurinol dispensed from a community pharmacy in three of four quarters of 2012. In the three years before 1 January 2012, 70% of both women and men with gout had serum urate tested at least once. Over the same period, 19.1% of women and 20.4% of men without gout had serum urate tested. Details on serum urate levels are presented in table 1.
Study participant characteristics (n=942 416)
Cardiovascular outcomes
People with gout had a much higher rate of first cardiovascular events (fatal and non-fatal) and higher non-cardiovascular mortality than people without gout. This observation was more pronounced in women than men (figure 2), largely because women with gout were considerably older than men with gout. For total cardiovascular events (fatal and non-fatal first cardiovascular events), we recorded 686 (11.0%) events in women with gout compared with 9869 events (1.9%) in women without gout, and 2185 (8.5%) events in men with gout compared with 12 788 (3.2%) events in men without gout. A total of 412 (6.6%) non-cardiovascular deaths in women with gout compared with 6531 (1.3%) in women without gout were recorded, with 1077 (4.2%) non-cardiovascular deaths in men with gout compared with 6836 (1.7%) in men without gout.

{kind=link}
{kind=link}
Kaplan-Meier curves for total cardiovascular events in women and men with and without gout
Multivariable Cox proportional hazards analyses
After adjustment for the cardiovascular predictors included in the sex specific models, gout was associated with an increased risk of a person experiencing a cardiovascular event over five years (adjusted hazard ratio 1.34 (95% confidence interval 1.23 to 1.45) in women; 1.18 (1.12 to 1.24) in men; table 2, model 1). The multivariable models without adjustment for gout or gout associated predictors are presented in online supplemental table 1. Significant interactions were identified between gout and ethnic origin in model 1 (online supplemental table 2A,B). The increased cardiovascular risk associated with gout was proportionally greater for men of Chinese, Indian, or other ethnic origins than for men of European, Māori, or Pacific Island ethnic origins. By contrast, although Māori women remain at highest risk of cardiovascular compared with other women, the increase in risk associated with gout was proportionally less than that for women of other ethnic groups. A significant interaction was also found between gout and sex in model 1 (adjusted hazard ratio 1.36 (95% confidence interval 1.24 to 1.48)).
Adjusted hazard ratios for fatal or first non-fatal cardiovascular events within five years in study population, according to sex. Data are adjusted hazard ratio (95% confidence interval)
Table 3 shows sex specific adjusted hazard ratios for regular dispensing of allopurinol (defined as allopurinol dispensed in three of four quarters of 2012; model 2); serum urate level (model 3); and dispensing of colchicine (model 4). The coefficients for established cardiovascular risk factors in multivariable models of time to first fatal or non-fatal cardiovascular event are not shown because they did not change measurably from model 1, with the addition of drug treatments for gout and serum urate level.
Effect of regular allopurinol dispensing, serum urate, and colchicine dispensing on adjusted hazard ratios for time to fatal or first non-fatal cardiovascular event within five years in study population, according to sex and analysis model. Data are adjusted hazard ratio (95% confidence interval)
We saw an increase in risk of cardiovascular events among men with gout who were not dispensed allopurinol in at least three of four quarters in the year after study entry compared with men with gout who were dispensed allopurinol (adjusted hazard ratio 1.15 (95% confidence interval 1.05 to 1.25); table 3, model 2). This effect was not observed among women. Among men with gout, we also saw a higher risk of cardiovascular disease associated with serum urate ≥0.36 mmol/L compared with serum urate <0.36 mmol/L (1.16 (1.04 to 1.30); table 3, model 3). This effect was also not observed in women.
Men with gout who were not dispensed colchicine at least once in the previous 12 months were found to be at lower risk of cardiovascular events than men with gout who were dispensed colchicine (adjusted hazard ratio 0.84 (95% confidence interval 0.77 to 0.92); table 3, model 4). In women with gout, we saw no difference in risk of cardiovascular events according to colchicine dispensing.
Discussion
Principal findings
In this large, representative, population cohort of adults with no history of cardiovascular disease in Aotearoa New Zealand, gout was associated with an increased occurrence of incident cardiovascular events in both sexes, after adjustment for multiple risk factors and preventive drug treatments at baseline. Regular dispensing of allopurinol and serum urate at target levels (<0.36 mmol/L) were associated with reduced risk of cardiovascular events in men with gout but not in women with gout. Colchicine dispensing was associated with increased risk of cardiovascular events in men with gout.
Comparison of findings with other studies
Our findings are consistent with the previous studies that have observed an association between gout and cardiovascular events.1–5 20 In the US Health Professionals Follow-Up Study, the relative risk of fatal cardiovascular disease was increased in men with gout compared with men without gout, after adjustment for other cardiovascular risk factors (adjusted relative risk 1.38 (95% confidence interval 1.15 to 1.66)).1 This study population was also a primary prevention cohort, but the cohort comprised well educated, predominantly white men (>90%) and might not be representative of the general population. An analysis using the All England National Linked Dataset from 1999 to 2011 found that the relative risk of myocardial infarction and stroke was increased in men and women with gout (in men: adjusted relative risk 1.73 (95% confidence interval 1.69 to 1.77) for myocardial infarction and 1.73 (1.69 to 1.78) for stroke; in women: 2.08 (2.01 to 2.16) for myocardial infarction and 1.71 (1.65 to 1.77) for stroke).20 However, this study was unable to adjust for dispensing of blood pressure lowering, lipid lowering, antiplatelet or anticoagulant, or gout drug treatments. Recently, a study investigating the Skåne Health Register in Sweden found that people with newly diagnosed gout had an increased risk of cardiovascular disease (adjusted hazard ratio 1.76 (95% confidence interval 1.69 to 1.84)).4 The authors included people with a history of cardiovascular disease, and found that gout was also associated with an increased risk of other conditions including renal disease, digestive diseases, infections, and dementia.
We found that gout modified the association between ethnic origin and cardiovascular events in both men and women. Men with gout and of Māori, Pacific Island, or Indian ethnic origin had a significantly higher risk of cardiovascular disease than men with gout from other ethnic groups. After accounting for this differential effect, Māori men with gout still remained at highest risk of cardiovascular disease, followed by Indian and Pacific Island men. A similar differential effect was observed among women. The risk of cardiovascular disease remains highest among Māori and Pacific Island people with gout. In Aotearoa New Zealand, Māori and Pacific Island people have the highest prevalence of gout,10 are least likely to be taking regular allopurinol,21 and have the highest burden of cardiovascular risk factors.22 With the additive risk factor of gout, our findings highlight the importance of resolving inequities in these population groups through access to timely and culturally safe care.23
In men with gout with no history of cardiovascular disease, we observed a reduction in cardiovascular risk in those individuals with regular allopurinol dispensing (dispensed in at least three of four quarters of 2012) and serum urate at target levels (<0.36 mmol/L), which suggests a possible cardiovascular benefit of appropriate gout management. These findings are similar to a study of the Multi-Payer Claims Database in the US, which found that in people with gout and diabetes, current allopurinol users had a significantly lower adjusted hazard of incident stroke or myocardial infarction than previous allopurinol users, (hazard ratio 0.67 (95% confidence interval 0.53 to 0.84)).14 Furthermore, in a cohort study of almost 1200 people with gout (92% men), researchers found that serum urate above the treatment target (≥0.36 mmol/L) was associated with an increased risk of cardiovascular disease and overall mortality.24 A meta-analysis of 32 studies (1 134 073 people) found a significant positive association between hyperuricaemia and risk of cardiovascular disease (adjusted hazard ratio 1.45 (95% confidence interval 1.33 to 1.58)), although heterogeneity between studies was high.25 By contrast, some earlier studies have not shown an association between hyperuricaemia and cardiovascular disease after adjustment for known cardiovascular risk factors.6–9 We are unaware of any published studies that have not shown an association between gout and cardiovascular disease.
The potential cardiovascular benefit of appropriate gout management (regular allopurinol dispensing and serum urate <0.36 mmol/L) among men in our cohort was not observed among women. Potentially in women, a lower target serum urate level could be required for cardiovascular benefit, with a study finding that the optimal discriminator level of serum urate for cardiovascular mortality was 0.30 mmol/L in women compared with 0.33 mmol/L in men.26 Non-linear modelling to explore the association between serum urate and cardiovascular disease in men and women will be undertaken in future studies.
Our study found that among people with no history of cardiovascular disease, colchicine dispensing (at least once in the past 12 months) was associated with an increased risk of cardiovascular events in men with gout. Recent large randomised controlled trials have shown that colchicine is beneficial for secondary prevention of cardiovascular disease (ie, in people with a history of cardiovascular disease).15 16 In the COLCOT trial, researchers found that patients randomised to receive colchicine 0.5 mg daily within 30 days after a myocardial infarction had a significantly lower risk of cardiovascular death, resuscitated cardiac arrest, myocardial infarction, stroke, or urgent hospital admission for angina leading to coronary revascularisation (adjusted hazard ratio 0.77 (95% confidence interval 0.61 to 0.96)).16 Similar findings were seen in the LoDoCo2 trial.15
The impact of colchicine has not previously been explored in people with no history of cardiovascular disease in randomised trials. In gout, colchicine is typically prescribed for a short period of time for the prevention or treatment of gout flares. People with gout who were dispensed colchicine are more likely to experience gout flares, which is associated with higher levels of systemic inflammation.27 This inflammation might mitigate the protective effects of colchicine in the setting of gout management. However, these findings need to be interpreted with caution, because the national dispensing database does not discriminate between the indication for colchicine dispensing (ie, short term use for gout flare treatment v longer term use for gout flare prophylaxis) and we did not observe the same association with colchicine dispensing and cardiovascular events in women.
Strengths and limitations of the study
This study of more than 940 000 participants explores the relation between gout and cardiovascular disease in a nationally representative population; our cohort identified almost all adults without cardiovascular disease in a geographical region that accounts for about a third of the total population in Aotearoa New Zealand. Strengths of our study included our use of predictors from prediction equations of cardiovascular risk developed from routinely collected administrative data, which have been validated within the adult population of Aotearoa New Zealand,17 to adjust our analyses. We also were able to analyse dispensing of gout specific drug treatments (allopurinol and colchicine) and serum urate levels through linkage to the national community pharmaceutical dispensing database and the Auckland/Northland regional repository of laboratory results. This linkage allowed us to use multiple surrogates for regular use of urate lowering treatment (dispensing of allopurinol in three of four quarters of 2012 and serum urate <0.36 mmol/L) to explore the relation between this treatment and cardiovascular risk.
Similar studies using linkage of administrative data have been conducted in the UK and in Sweden.4 20 However, these previous studies did not account for cardiovascular risk factors, drug dispensing, or serum urate levels at baseline. Furthermore, in the Swedish study,20 the cohort included people with previous cardiovascular disease. Our study used ICD coded diagnoses to identify and exclude those individuals with a history of cardiovascular disease over an extended period (1988-2011). This approach has been validated in European countries28–30 and previous national cardiovascular studies in Aotearoa New Zealand.17 31 We used a broad definition for cardiovascular disease, reducing the likelihood that relevant diagnoses were missed. The clinical coding is performed by qualified medical coders within each District Health Board of Aotearoa New Zealand, leading to improved consistency compared with systems where coding data is entered ad hoc by clinicians. Although individuals receiving a diagnosis of cardiovascular disease solely in primary care or the private healthcare sector would not have been captured by this definition, private hospital admissions account for less than 2% of admissions for acute ischaemic heart disease in Aotearoa New Zealand.31 Our definition of cardiovascular disease identified diagnoses that were severe enough to warrant hospital admission or result in death, which accounts for the most definitive diagnoses. Furthermore, patients with cardiovascular disease who used private healthcare are likely, at some stage, to have contact with acute, publicly funded, hospital cardiac services where diagnostic data would be captured.
The methodology for defining gout used in our study has been validated against the primary care diagnosis of gout10 as well as microscopic crystal identification.32 The definition has been routinely used to evaluate the prevalence of gout in Aotearoa New Zealand over the past decade,10 21 33 and in an insured population in the US.34 The choice between non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids, or colchicine for the treatment of gout flares depends on patient preference, comorbidities (renal or liver impairment, previous cardiovascular disease, peptic ulcer disease, diabetes, infection, fluid overload), and concomitant drug treatments (anticoagulants, P glycoprotein inhibitors, CYP3A4 inhibitors).35 Although we could have excluded people with gout who were only treated with NSAIDs or corticosteroids, these drugs were not included in the gout definition because they are not specific to gout and could have been dispensed in people with gout for other non-gout indications. How this definition might have affected our study findings is unclear because we are unable to ascertain the rationale for the dispensing of NSAIDs, corticosteroids, or colchicine from the national database of community pharmaceutical dispensing.
We used this approach to ensure that we were capturing only people with gout and to minimise potential confounding from comorbidities and concomitant drug treatments that we were unable to adjust for. This approach has been estimated to undercapture up to 20% of gout cases in Aotearoa New Zealand.36 Time related biases have been recognised in previous observational studies of allopurinol on mortality.37 In our study, people with defined gout were identified before the start of follow-up (before 1 January 2012) to avoid immortal time bias and we minimised immeasurable time bias, by using a surrogate of allopurinol adherence (dispensed in three of four quarters of one year) rather than once-off dispensing of allopurinol.
We were unable to adjust our analyses for some known modifiable risk factors for cardiovascular disease, such as blood pressure, lipid levels, body mass index, and smoking status, which are not recorded in the national, routinely collected, health administrative data. However, consistent with the risk equations for cardiovascular disease developed from Aotearoa New Zealand national data, we used dispensing of blood pressure lowering and lipid lowering drugs as surrogates for blood pressure and lipid levels.17 Age also acts a proxy for the length of exposure to multiple cardiovascular risk factors.38
We were also unable to adjust for chronic kidney disease, which has been shown to be associated with increased risk of gout, particularly in women.39 We used regular dispensing of allopurinol in three of four quarters of 2012 as a surrogate for regular use of drug treatment but cannot be certain that people with gout who were dispensed allopurinol might have actually taken this drug or continued taking it during follow-up. Similar approaches to assess adherence from community pharmaceutical dispensing data have been used for metformin,40 statins, and antihypertensive drugs.41 Nevertheless, the findings of our study demonstrate an association between gout and cardiovascular disease. The potential causal mechanisms of these associations require further exploration including casual inference modelling in future studies.
Conclusion
Gout is associated with an increased risk of both fatal and non-fatal cardiovascular events. In men with gout with no history of cardiovascular disease, regular allopurinol dispensing and serum urate levels at standard treatment targets was associated with a lower risk of cardiovascular disease. By contrast, colchicine dispensing was associated with an increased risk of cardiovascular events in men with gout with no history of cardiovascular disease.
Data availability statement
Data are available upon reasonable request. All individual participant (deidentified) data, including a data dictionary defining each field, will be made available to university based academic researchers if their proposed analyses are approved by the investigators’ data access proposal committee. A proposal must be considered relevant to the original aims of the research, must meet the study's ethics approval criteria, and will require one or more of the study investigators as formal collaborators. A signed data access agreement will be required and the costs of preparing the datasets will need to be covered. There are no set dates for when these data will be made available. Please contact the corresponding author regarding data sharing requests.
Ethics approval
This study involves human participants and was approved by Northern Region Ethics Committee Y in 2003 (AKY/03/12/314), with subsequent annual re-approval by the national Multi-Region Ethics Committee since 2007 (MEC/01/19/EXP). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KC, ND, KP, and RJ conceptualised and designed the study. KC, BW, and KP were involved in the data collection process. KC analysed the data with input from RJ, KP, SM, and BW. All authors were involved in data interpretation. KC, ND, and KP drafted the manuscript and all authors revised the manuscript. All authors approved the final submitted version and agreed to be accountable for the report. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication. KC, BW, and KP have directly accessed and verified the data. KC and KP are the study guarantors. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. Transparency: The lead author (the guarantor) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Funding This study was funded by the Health Research Council of New Zealand and Arthritis Australia. The study funders had no role in the study design, collection, analysis, or interpretation of data. The views expressed in this publication are those of the author(s) and not necessarily those of the funding bodies.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from Health Research Council (HRC) of New Zealand and Arthritis Australia for the submitted work; KC reports a research fellowship grant from Arthritis Australia; SM reports a research grant from the HRC VIEW programme and HRC Clinical Research Training Fellowship; ND reports grants and personal fees from AstraZeneca, grants from Amgen, personal fees from Dyve, personal fees from Hengrui, personal fees from Horizon, personal fees from Selecta, personal fees from Abbvie, personal fees from Arthrosi, personal fees from Janssen, outside the submitted work; KP reports a grant from the Heart Foundation Hynds Senior Fellowship; SMW reports a grant from the Health Research Council of New Zealand and the Stevenson Foundation; CG reports a grant from the Heart Foundation and Healthier Lives (National Science Challenge); the other authors declare no conflicts of interest.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.