Article Text

Abstract
Objective To determine the effect of covid-19 vaccination, given before and after acute infection with the SARS-CoV-2 virus, or after a diagnosis of long covid, on the rates and symptoms of long covid.
Design Systematic review.
Data sources PubMed, Embase, and Cochrane covid-19 trials, and Europe PubMed Central (Europe PMC) for preprints, from 1 January 2020 to 3 August 2022.
Eligibility criteria for selecting studies Trials, cohort studies, and case-control studies reporting on patients with long covid and symptoms of long covid, with vaccination before and after infection with the SARS-CoV-2 virus, or after a diagnosis of long covid. Risk of bias was assessed with the ROBINS-I tool.
Results 1645 articles were screened but no randomised controlled trials were found. 16 observational studies from five countries (USA, UK, France, Italy, and the Netherlands) were identified that reported on 614 392 patients. The most common symptoms of long covid that were studied were fatigue, cough, loss of sense of smell, shortness of breath, loss of taste, headache, muscle ache, difficulty sleeping, difficulty concentrating, worry or anxiety, and memory loss or confusion. 12 studies reported data on vaccination before infection with the SARS-CoV-2 virus, and 10 showed a significant reduction in the incidence of long covid: the odds ratio of developing long covid with one dose of vaccine ranged from 0.22 to 1.03; with two doses, odds ratios were 0.25-1; with three doses, 0.16; and with any dose, 0.48-1.01. Five studies reported on vaccination after infection, with odds ratios of 0.38-0.91. The high heterogeneity between studies precluded any meaningful meta-analysis. The studies failed to adjust for potential confounders, such as other protective behaviours and missing data, thus increasing the risk of bias and decreasing the certainty of evidence to low.
Conclusions Current studies suggest that covid-19 vaccines might have protective and therapeutic effects on long covid. More robust comparative observational studies and trials are needed, however, to clearly determine the effectiveness of vaccines in preventing and treating long covid.
Protocol registration Open Science Framework https://osf.io/e8jdy.
- covid-19
Data availability statement
No additional data available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Long covid is a serious new public health problem, and how vaccination against covid-19 disease affects patients with long covid is unclear
WHAT THIS STUDY ADDS
No randomised controlled trials have assessed the effect of covid-19 vaccination on preventing or treating long covid
Data from 16 observational studies suggest that covid-19 vaccination could protect against long covid
Observational studies suggest that vaccination might help those with a diagnosis of long covid
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE, OR POLICY
More robust comparative observational studies and trials are needed to clearly determine the effectiveness of vaccines in preventing and treating long covid
Introduction
Long covid, also known as post-acute covid-19 sequalae or post-acute covid-19 syndrome, is recognised as a major concern after infection with the SARS-CoV-2 virus, and will likely cause substantial global morbidity for many years.1 2 With global numbers of infections of more than 500 million and a conservative prevalence of 20-30%, more than 100 million people could be currently affected by long covid worldwide.3–5
In October 2021, the World Health Organization defined long covid as symptoms occurring in people with a history of probable or confirmed SARS-CoV-2 infection, usually within three months, and lasting for at least two months, that cannot be explained by an alternative diagnosis.6 7 Many symptoms associated with long covid have been reported that can last for months, and the common symptoms include, but are not limited to, fatigue, cognitive dysfunction, head, body, and joint pains, and dyspnoea.8 9 Factors such as female sex, severe initial disease, and comorbid conditions seem to be associated with the risk of long covid.10
Interest in the effect of covid-19 vaccination on long covid has been growing.2 11 Recent observational studies give contradictory results, however, and have methodological flaws, which preclude firm conclusions on the effect of vaccination on long covid.12 13 The covid-19 vaccines could work on three levels to prevent or treat long covid: firstly, by preventing infection with the SARS-CoV-2 virus; secondly, by reducing the severity of the disease in people who have been vaccinated and are then infected with the virus; and thirdly, by benefiting people who already have long covid. Hence the aim of our study was to assess the effect of covid-19 vaccination, given before and after acute infection with the SARS-CoV-2 virus, and also after a diagnosis of long covid, on the rates and symptoms of long covid.
Methods
We conducted a systematic review with enhanced processes and automation tools.14 The systematic review is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.15 Our protocol was shared on the Open Science Framework (https://osf.io/e8jdy) on 2 March 2022.
We searched the PROSPERO and Open Science Framework databases to exclude similar reviews. We then searched PubMed, Embase, and Cochrane covid-19 trials for published studies, and Europe PubMed Central (Europe PMC) for preprints, from 1 January 2020 to 3 August 2022. A search string of medical subject headings terms and words was developed in PubMed and translated to run in other databases with the Polyglot search translator.16 Online supplemental file 1 shows the search strategies for all databases.
Supplemental material
We also conducted forward and backward citation searches of the included studies. For registered studies, we searched ClinicalTrials.gov and the WHO International Clinical Trials Registry Platform. Searches were run from inception to 3 August 2022 (appendix 1). We also checked the VIEW-hub database (www.view-hub.org), a collaboration between the International Vaccine Access Centre and Johns Hopkins Bloomberg School of Public Health. No publication type or language restrictions were applied. We also contacted authors of large vaccine trials for any unpublished data on long covid.
We included randomised controlled trials, cohort studies (retrospectively or prospectively assembled), interrupted time series, and case-control studies. We excluded case reports, case series, cross sectional studies, and modelling studies. We searched for studies that assessed vaccination status and the emergence of long covid (history of confirmed or probable covid-19 within the past three months and symptoms that lasted at least two months that could not be explained by an alternative diagnosis). Studies conducted in the community, primary care, and hospital settings were included.
Our inclusion criteria were people of all ages who were eligible to receive a covid-19 vaccine. The interventions were any dose of a covid-19 vaccine recognised by WHO (ie, BNT 162b2 (tozinameran, Pfizer-BioNTech), mRNA-1273 (elasomeran, Moderna), ChAdOx1 nCoV-19 (Oxford-AstraZeneca), and Ad26.COV2.S (Janssen or Johnson & Johnson)), before or after the first SARS-CoV-2 infection, or after a diagnois of long covid. Comparators were no vaccination, an active non-covid-19 vaccine control (eg, influenza vaccine), or placebo.
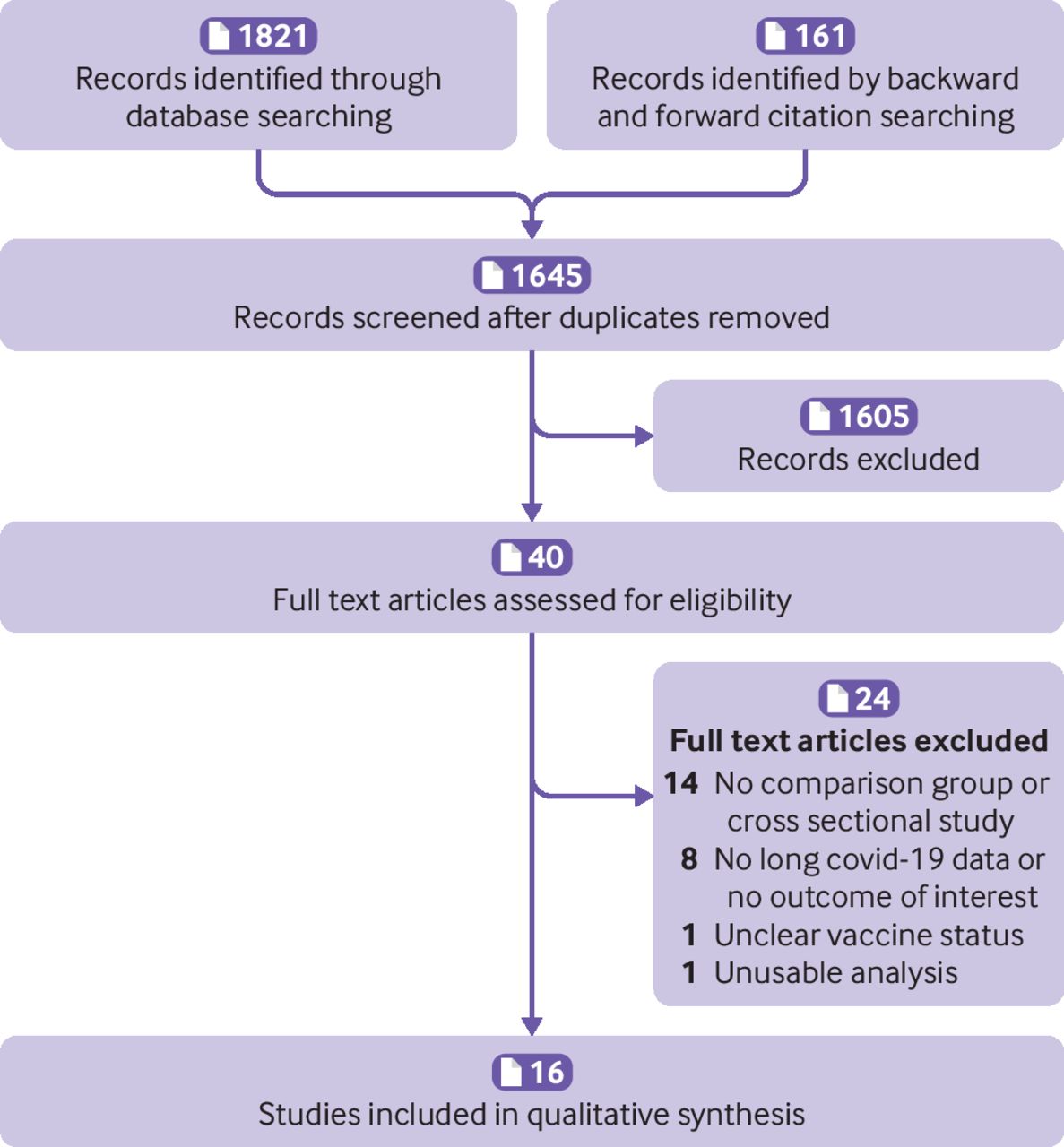
The primary outcomes were patients with a diagnosis of long covid, according to the WHO definition (ie, history of confirmed or probable covid-19 within the past three months and symptoms that lasted at least two months that could not be explained by an alternative diagnosis), and remission or resolution of long covid in patients who were vaccinated after a diagnosis of long covid. The secondary outcome was prevalence of individual symptoms of long covid, such as prolonged fatigue, shortness of breath, cognitive difficulties, and loss of sense of smell. We excluded protocols, studies that did not report long covid outcomes, and studies with uncertain vaccination status at the time of infection (figure 1).
Screening and selection of studies
Study selection and screening
Two of the authors (OB and PS) independently screened the titles and abstracts, and full text articles were retrieved for potentially eligible articles. The full texts were then reviewed against the inclusion criteria. Discrepancies were resolved by referring to a third author (PG). Figure 1 summarises the screening process. Online supplemental file 2 lists the excluded articles and reasons for exclusion.
Data extraction
Two of the authors (OB and PS) extracted the data with Microsoft Excel. Study characteristics and outcomes extracted from each study were: methods (study authors, year, country, study design, length of follow-up, and setting); participants (number of participants, age, sex, and any co-comorbidities); interventions (type of intervention, dose, and frequency) and type of comparators (no treatment, other non-covid-19 vaccine, or placebo); and outcomes (patients with long covid (primary outcome) and prevalence of individual symptoms (secondary outcome)).
Assessment of risk of bias
Risk of bias was assessed with the ROBINS-I tool, which can assess both randomised and non-randomised studies on a common template.17 Two of the authors (OB and PS) independently assessed the risk of bias for each study.
Data analysis
We did not conduct meta-analyses because of the high heterogeneity of the data. For dichotomous outcomes, the effect of the intervention was calculated with odds ratios. For one study, we calculated the odds ratio from the reported mean differences.18 We used individual participants as the unit of analysis. When data were missing or unclear, the study investigators were contacted. We found no registered trials for vaccines and long covid. We could only present subgroups by dose of vaccine and timing of vaccine dose.
Patient and public involvement
Patients and the public were not involved in this review. Systematic reviews identify and analyse relevant primary studies to answer a specific research question, but they are not conducted on patients or public directly. We plan to disseminate our results through open access publication, our institute’s monthly newsletter, and preprint database update.
Results
Of 1645 titles and abstracts screened, 40 full text articles were assessed for inclusion (figure 1). We found no eligible randomised trials. The 16 eligible observational studies (including seven preprints) were based on data from five countries (USA (n=8), UK (n=4), the Netherlands (n=2), France (n=1), and Italy (n=1)) that included 614 392 patients19–34 (tables 1 and 2). Online supplemental file 2 lists the articles that were excluded and the reasons for exclusion.
Characteristics of included studies of vaccines given before infection
Characteristics of included studies when vaccines were given after infection or after a diagnosis of long covid
Eleven studies assessed the effect of a vaccine given before infection with the SARS-CoV-2 virus19–29 (table 1); four studies assessed the effects of a vaccine after infection and after a diagnosis of long covid30 32–34 (table 2). One study provided data for both vaccination before and after infection and therefore was included in both tables.31 Five of the studies used data from three large medical databases,19 23 27 29 31 five studies used the covid-19 symptom study app user data or national covid-19 survey data,20 21 25 28 30 two studies involved healthcare workers and professionals,22 24 and four studies recruited patients who already had symptoms of long covid to prospectively follow for remission or recovery.30 32–34
All but one study was conducted and concluded by December 2021, and thus did not include data on the omicron variant of the SARS-CoV-2 virus.22 Only one study cited the current case definition of long covid by WHO.34 Five studies did not provide a clear definition of long covid but reported 3-6 months of follow-up outcomes.19 21 23 25 28 Five studies used symptoms lasting longer than 28 days since the onset of acute infection as the cut-off for long covid.20 22 26 29 30 Nine studies used self-reported symptoms as a diagnosis of long covid,20–22 24 28 30 32–34 five studies used ICD-10 (international classification of diseases, 10th revision) codes to determine organ-system symptoms related to long covid to establish the presence of long covid,19 23 27 29 31 one study used electronic health record data,26 and one study used a combination of patient self-report and ICD-10 codes.25
Secondary outcomes were reported in four studies.20 25 26 30 The most common symptoms of long covid were fatigue, cough, weakness and tiredness, loss of sense of smell, shortness of breath, loss of taste, headache, difficulty sleeping, difficulty concentrating, muscle ache, worry or anxiety, and memory loss or confusion.
Effect of vaccination on outcomes of long covid
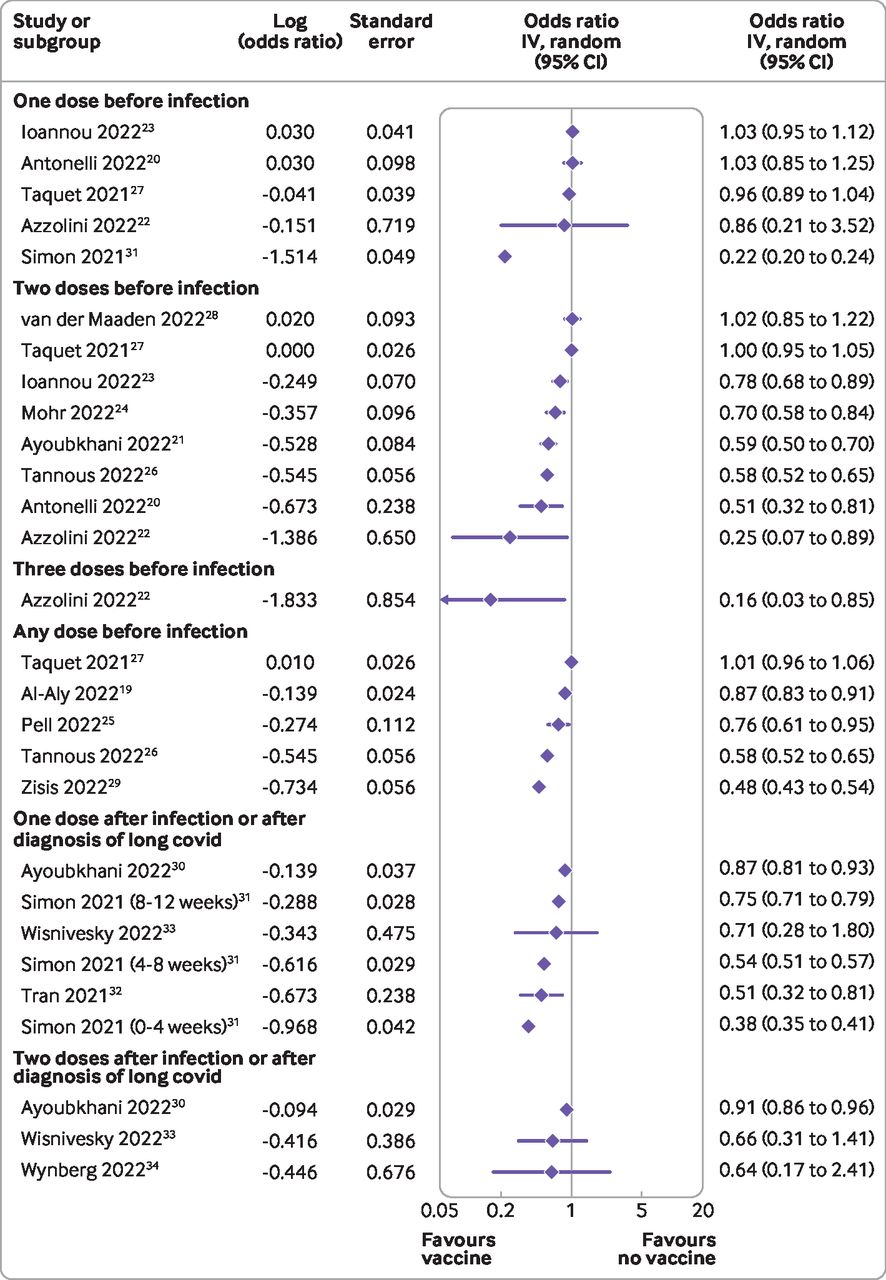
The high heterogeneity between studies precluded a meaningful meta-analysis. The forest plot of the outcomes of each study showed high heterogeneity (figure 2). Twelve studies reported data on vaccination before infection with the SARS-CoV-2 virus,19–29 31 of which 10 showed a significant reduction in the incidence of long covid.19–26 29 31 The odds ratio of developing long covid with one dose of vaccine before infection ranged from 0.22 to 1.03; for two doses, odds ratios were 0.25-1.02; and with any dose of vaccine before infection, the odds ratio was 0.48-1.01. One study reported the odds of having long covid at one month after infection with three doses of vaccine (odds ratio 0.16, 95% confidence interval 0.03 to 0.85).22 The five studies that reported data on vaccination after infection had odds ratios ranging from 0.38 to 0.91. Two studies that assessed remission32 and recovery34 from long covid reported the odds of not recovering when patients were vaccinated after infection as 0.51 (95% confidence interval 0.32 to 0.81) and 0.64 (0.17 to 2.33), respectively. Online supplemental file 3 shows all ratios and their explanations, along with timeframes.
{kind=link}
{kind=link}
Forest plot of the effect of covid-19 vaccine doses on long covid. Only relevant outcomes from all reported outcomes in individual studies were chosen. The ratios have a range of time frames (tables 1 and 2, and online supplemental file 3). IV=inverse variance
Risk of bias in included studies
The risk of bias of the included studies was assessed by the ROBINS-I tool for non-randomised studies of interventions. The risk of bias of the individual studies was judged overall as moderate to critical. The primary sources of increased bias were domains that dealt with confounding, missing data, and measurement of outcomes. The main concerns arising from confounding were not accounting for vaccine hesitancy or severity of the original disease. Most of the studies did not report on how missing data were dealt with.
Bias in measurement of outcomes was rated moderate to critical in studies where the exposure (vaccination) and outcome measurements (symptoms of long covid) were collected together, or where participants were aware of their exposure at the time of the measurement and thus the reporting of the outcome could be potentially influenced by that knowledge. Another reason for the increased bias in outcome measurements was the unclear definition of long covid, particularly in studies that analysed data from electronic health record databases (table 3). Online supplemental file 4 provides further methodological details of the included studies.
Risk of bias in included studies assessed by the ROBINS-I tool
Discussion
Principal findings
We found no randomised controlled trials, but 16 observational studies provided outcomes on long covid. Six of the eight studies of two or more doses of vaccine given before infection with the SARS-CoV-2 virus found significant reductions in the rates of long covid. A similar result was less clear with only one dose of vaccine. Three of the five studies of vaccination after the infection showed significant reductions in patients with long covid, but none showed any harm of vaccination. Owing to insufficient data, we could not examine any dose-response association. All 16 studies were non-randomised, and most were assessed as having a moderate to critical risk of bias. Thus the evidence summarised here is of low certainty.
Strengths and weaknesses of the study
The strengths of our review were the search of multiple databases for published (including preprints) and unpublished articles, and public health reports. We critically assessed the risk of bias of the included studies to identify the main sources of bias.
Our study had several limitations. The greatest challenge in conducting this review was the validity of the diagnoses of long covid in the included studies. Most studies established a diagnosis of long covid based on the length of time symptoms were reported by participants or on data from electronic health records and ICD-10 codes, rather than from healthcare professionals, as anticipated. The studies also used different cut-off times for long covid; the shortest was 28 days. After infection with the virus, many symptoms, such as fatigue, routinely last more than a month.35 Although the WHO Delphi consensus on the definition of long covid was much needed, lack of awareness of the definition by health professionals might be hindering the diagnosis of long covid and therefore real world data on long covid.
Furthermore, we could not recalculate a common ratio for most of the studies and so we plotted relative risk ratio, odds ratio, and hazard ratio reported by the studies together as a close approximation.36 Also, we could not conduct a meta-analysis of the studies because of the high heterogeneity and lack of data on the types of vaccines, time between exposure and disease, and variants of the virus, highlighting the need for standardisation and validation studies of outcome measures for ongoing research on long covid.
Another limitation was that not many of our included studies reported on our secondary outcome, prevalence of individual symptoms of long covid. Several studies showed changes in symptoms after vaccination, but they were mostly cross sectional in design and thus establishing true causality was not possible; these studies were excluded. Furthermore, the characteristics and symptomatology of long covid are becoming well established with global data.1 5 37
Strengths and weaknesses in relation to other studies
One systematic review,38 one scoping review,39 and two government reports (by Public Health Ontario and UK Health Security agency) estimated the effect of vaccination on long covid.40 41 The government reports were rapid reviews and therefore a rigorous search or quality assessments on the reported studies was not done. All four studies included multiple cross sectional studies and only narratively explained the findings. Because of the lack of rigorous inclusion criteria, these reviews cannot be used to establish the effectiveness of vaccines in preventing long covid. Our review also includes more up-to-date evidence.
Meaning of the study
Vaccines against covid-19 disease have been found to prevent infection in patients, particularly for the earlier variants of the SARS-CoV-2 virus, and so would prevent long covid by preventing the initial infection. Less clear, although highly plausible, has been whether vaccines, by reducing the severity of symptoms of covid-19, reduce the prevalence of long covid after infection. The studies we identified were inconsistent, although the results showed a tendency towards vaccines reducing the prevalence of long covid. Vaccination after infection and in those with long covid has been more controversial, but the studies we identified are reassuringly consistent in being protective.
Unanswered questions and future research
A key finding of this review was the lack of high quality studies, particularly randomised trials, to determine the effect of vaccines on long covid. This finding has several implications for future research. Firstly, the best data on the effect of vaccines in patients with long covid after breakthrough infections (ie, infections that occur after vaccination) could have come from large clinical trials of vaccines. Our search for these data showed that trials on the efficacy of vaccines did not plan or collect suitable data for these outcome. Designing follow-up studies of breakthrough infections from ongoing vaccine trials to estimate rates of long covid is still possible.
Secondly, ongoing trials on the effectiveness of vaccines in children should include provisions for longer follow-up of patients who are infected with the virus after vaccination. Thirdly, the studies included in our review were conducted up to December 2021 and so do not include data on the omicron variant of the SARS-CoV-2 virus. Data from the UK Office for National Statistics found that the omicron variant of the virus caused the greatest number of patients with covid-19 and long covid in the UK.42 But a new analysis that compared the periods in the UK when the delta and omicron variants of the SARS-CoV-2 virus were the most prevalent, showed that during the omicron wave, the prevalence of long covid was about half that in previous waves, and patients infected with the omicron variant were less likely to have long covid even with more than six months between vaccination and infection (odds ratio 0.24-0.50).43
Mapping long covid data to the different subvariants of the SARS-CoV-2 virus will also help inform public health measures against the spread of the pandemic. In the meantime, researchers should use trial emulation techniques to better estimate the effect of vaccines on different age groups and variants. In our review, only one study explicitly emulated a target trial27 and less than half used propensity score matching when creating their comparator cohorts.19 21 29 32–34
Fourthly, the data from our included studies also suggested that covid-19 vaccines at least provide equipoise in terms of prevention and treatment of long covid, and thus trials on the effect of vaccination in patients after infection and after a diagnosis of long covid should be conducted as a priority. Although vaccine coverage might seem high in many western countries, several studies reported vaccine hesitancy in patients with long covid (>50%) because of fear of worsening symptoms and the belief that covid-19 vaccines were contraindicated in long covid.44 45 Finally, awareness of the case definition of long covid by medical professionals and management in parallel with the care needs of patients with long covid should be explored.
Conclusions
Covid-19 vaccines have saved millions of lives and prevented severe forms of the disease. The effect of the vaccines on preventing or treating long covid, however, was not conclusively established in this review. Many questions need to be answered as a priority, which will require agreed standards for outcomes, improved methods and analysis, better reporting, and application of these questions to current and future studies. This approach is particularly important for ongoing or new trials where consent should be obtained for follow-up of symptoms of long covid.
Data availability statement
No additional data available.
Ethics approval
Not applicable.
Acknowledgments
We thank the authors of the eligible papers for their replies to our queries. We also thank David Henry for his methodological expertise on the risk-of-bias assessment.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @OyukaMDPhD
Contributors PG conceived the study and co-designed the study with OB, PS, and KA. JC led the literature searches including backward and forward citation analysis. OB and PS conducted the parallel title, abstract, and full text screening. OB and PS did data extraction and analysis. All authors contributed to resolving disagreements throughout the study and to writing of the manuscript. PG is the guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. Transparency: The lead author (the guarantor) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.