Article Text

Abstract
Objective To assess and clarify the relations between selective serotonin reuptake inhibitor (SSRI) dose efficacy, acceptability (early treatment discontinuation (dropouts)), and tolerability (reported adverse drug effects), and critically evaluate methods previously used to examine SSRI dose-response effects for the treatment of depression in adults.
Design Systematic review of reviews and meta-narrative synthesis.
Data sources Embase, Medline, PsycINFO, Scopus, and the Cochrane Collaboration library, from 1975 to December 2021. Reference lists of national depression treatment guidelines were systemically searched by hand.
Eligibility criteria for selecting studies Reviews assessing SSRI monotherapy dose-response effects for the treatment of depression in adults (age ≥18 years) reporting efficacy, acceptability, or tolerability. Reviews meeting inclusion criteria had a high degree of heterogeneity, due to methodological diversity; therefore, a meta-narrative synthesis approach was applied. Standard daily doses were defined as 20 mg citalopram, fluoxetine, paroxetine; 50 mg sertraline; and 10 mg escitalopram. Risk of bias was assessed using the Risk of Bias in Systematic Reviews tool, in line with Cochrane recommendations.
Results The search identified 9138 records; 387 full text reports were assessed for eligibility, 42 of which matched the inclusion criteria. The majority, 83% (n=35), of reviews included data for studies with a duration of ≤12 weeks (ie, the acute phase of depression treatment). Of 39 reviews assessing efficacy, the majority (n=26) indicated that individual SSRIs and SSRI class demonstrated flat dose-response effects; standard doses were optimal for efficacy. Acceptability or tolerability were assessed in 28 reviews. Higher than standard daily doses were associated with higher dropout rates and a greater incidence of adverse drug effects (eg, nausea, sexual dysfunction, fatigue, anxiety). Despite a range of methods being reported, there was an overall consensus regarding SSRI dose related efficacy, dropouts, and adverse drug effects.
Conclusion Standard daily doses of SSRIs for the treatment of depression in adults provide a favourable balance between efficacy, acceptability, and tolerability. Patients are encouraged to talk to their prescriber or community pharmacist if they experience adverse effects or have any concerns about their drug treatments.
- Mood disorders
- Psychiatry
- Pharmacology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Selective serotonin reuptake inhibitors (SSRIs) are the most commonly prescribed antidepressants for depression treatment worldwide
In recent years, higher doses of SSRIs are being used to treat depression
It is unclear whether SSRIs show a dose-response effect for efficacy in depression treatment, and most clinical guidelines lack clarity regarding antidepressant dose-response effects
Use of higher SSRI doses could expose people to avoidable drug related harms without providing greater efficacy
WHAT THIS STUDY ADDS
Standard daily doses (20 mg citalopram, fluoxetine, paroxetine; 50 mg sertraline; and 10 mg escitalopram) provide a favourable balance between efficacy, acceptability, and tolerability, in the acute phase of treatment
Higher than standard daily doses were associated with higher dropout rates and a greater incidence of adverse drug effects (eg, nausea, sexual dysfunction, fatigue, anxiety)
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE, OR POLICY
There is a lack of primary studies assessing the dose-response effects in older adults who are commonly prescribed SSRIs
Routinely increasing SSRI doses for individuals not achieving satisfactory symptom resolution or remission does not appear to be supported by current evidence
Prescribers might find these findings of use when discussing antidepressant dose limitations and harms with patients
Clearer inclusion of antidepressant dose-response effects and efficacy limitations in clinical guidelines could help to better optimise outcomes while minimising avoidable drug related harms
Introduction
Selective serotonin reuptake inhibitors (SSRIs) are the most commonly prescribed antidepressants around the world, accounting for more than 50% of all antidepressant prescriptions.1–4 Most SSRIs are prescribed for the treatment of depression.5 6 Over recent years, use of higher than standard licensed SSRI doses for depression treatment has increased in UK primary care and elsewhere.5 7–9
SSRIs exert their effects via serotonin reuptake inhibition, and have a hyperbolic association between dose, transporter occupancy, and plasma concentration with SSRI doses of 20 mg citalopram, fluoxetine, paroxetine; 50 mg sertraline; and 10 mg escitalopram; with daily doses providing optimal receptor occupancy and serotonin effects.10 Therefore, the theoretical rationale for increasing standard daily doses of SSRIs for individuals not achieving satisfactory symptom resolution or remission are scarce. Conversely, tricyclic antidepressants and serotonin and noradrenaline (norepinephrine) reuptake inhibitors (SNRIs) have shown serotonin, norepinephrine, and dopamine effects as doses are increased.11 12 For example, venlafaxine shows predominantly serotonin effects at doses <150 mg per day, with norepinephrine effects becoming clinically significant from ≥150-225 mg per day, and dopamine reuptake inhibition from >225 mg per day.12 Therefore, tricylic antidepressants and SNRIs demonstrate dose-response effects for efficacy owing to their multiple receptor effects with higher doses being more effective where they are tolerated.13 14
Over the past 20 years numerous reviews have assessed antidepressant efficacy,15 ,16 17 however, few have assessed dose-response effects. These reviews have shown a mixed picture—some have indicated that higher than standard initiating doses are more efficacious,18 19 while others have refuted this finding,13 20 demonstrated mixed effects,21 or remained ambiguous.22 In part, some of these differences in findings might be due to newer analytical methods being more comprehensive and robust; but newer reviews also show mixed findings.18–20 23 However, some reviews agree that higher doses are associated with more adverse drug effects.13 19 21–23
This ambiguity regarding SSRI dose-response and efficacy feeds into national guidelines for depression treatment in Europe, North America, and Australasia, where few highlight the possible limitations of increasing SSRI doses,24 25 and lack clarity (see online supplemental table S1).26 ,27 28 Clinicians might therefore decide to increase SSRI doses routinely, and while in part this increase could be due to the doses used in clinical trials and different prescribing cultures (ie, higher SSRI doses more commonly prescribed in North American trials compared with European studies29 30), it might also be in response to some patients’ expectations of higher doses being more effective.31 However, whether increasing SSRIs doses provides greater efficacy for the treatment of depression remains unclear. Therefore, this systematic literature review of reviews aimed to assess and clarify the relation between SSRI dose for efficacy (response and/or remission), acceptability (early treatment discontinuation—dropouts) and tolerability (reported adverse drug effects), and critically evaluate the methods previously used to examine SSRI dose-response effects for the treatment of depression in adults.
Supplemental material
Methods
Study design
Recommendations from the Cochrane Handbook for Systematic Reviews of Interventions informed the design of this systematic review.32 This systematic review was conducted according to the PRISMA (preferred reporting items for systematic reviews and meta-analyses) 2020 checklist.33 The publicly available protocol for this review of reviews is available on the institutional website of University of Stirling (http://hdl.handle.net/1893/33209). Previous reviews have applied a diverse range of review methodologies to assess SSRI dose-response effects; therefore, we applied a meta-narrative synthesis approach for this review of reviews.
This systematic meta-narrative synthesis is reported in compliance with PRISMA and RAMESES (realist and meta-narrative evidence syntheses: evolving standards).33 34 The updated PRISMA flow chart was used to outline study selection process used to identify reviews which met the inclusion criteria.33 A meta-narrative review is a method of systematic review, designed for topics that have been conceptualised differently and studied by different groups of researchers. A meta-narrative synthesis brings together the studies that have been differently conceptualised by different researchers.34
Search strategy and criteria of eligibility and inclusion
The inclusion criteria for this systematic review and synthesis are presented according to PICOS (population, intervention, comparator, outcomes, study design) criteria (table 1).
PICOS inclusion criteria
Population
We included literature reviews for adults aged ≥18 years with depression. Depression was used as the common summary term that included: major depressive disorder, unipolar depression, depressive disorder, endogenous depression, and organic depression. Diagnostic criteria and severity of depression were not defined because primary studies were not being assessed. We considered a broad age range appropriate owing to the common trend of ageing populations across westernised societies, and about 20% of older adults (aged ≥65 years) receiving antidepressants in the UK and US.1 4 35
We excluded reviews of children and adolescents aged <18 years with depression, because this cohort is not routinely treated in primary care by general practitioners and have variable response rates to antidepressants.36 Reviews including older people with dementia were excluded because antidepressants have questionable benefits for depressive symptoms in this cohort.37 Additionally, owing to differences in disorder causes, bidirectional effects between depression and comorbidities, and previous evidence of treatment resistance, we excluded the following criteria: treatment resistant depression, depression during pregnancy, perinatal depression, postnatal depression, bipolar disorder, concomitant psychiatric disorders, people who use drugs, concomitant opioid replacement treatment, or specific comorbidities (eg, diabetes, post-myocardial infarction).38–41
Interventions and comparators
Reviews assessing SSRI monotherapy for the treatment of depression for all licensed SSRIs were included: citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline. The SSRI zimelidine was not included because it has been withdrawn from the market, owing to its use being associated with Guillain-Barré syndrome.42 Antidepressants outside the SSRI class with novel serotonin or mixed receptor effects were excluded: vortioxetine is a direct modulator of serotonergic receptor activity and inhibitor of serotonin reuptake; vilazodone has mixed SSRI and buspirone-like activity; the SNRIs venlafaxine and duloxetine; the tricyclic antidepressant clomipramine; and bupropion and agomelatine.43–45
Reviews examining combination treatments (using two or more antidepressants; psychotropic and non-psychotropic medicine augmentation strategies; antidepressant with psychotherapies; and switching antidepressants) were excluded because these strategies can be more effective than monotherapy and can be reserved for treatment resistant depression.24–28 Most national guidelines24–28 and drug licenses recommend standard starting doses,43 which are routinely prescribed in practice,5 9 46 47 and represent standardised defined daily doses as defined by the World Health Organization.48 It was therefore considered appropriate to assess baseline standardised comparator dose effects against placebo and higher SSRI doses, but owing to the range of methodologies and reporting methods, it was not possible to summarise the magnitude of effects using defined daily doses.
Outcomes
These outcomes were defined as dose-response effects for efficacy, acceptability, tolerability. Efficacy was defined as a response to antidepressant treatment, which is routinely defined as a ≥50% reduction in observer rated depression severity rating scales such as the Hamilton depression rating scale, Montgomery-Ǻsberg depression rating scale, or Beck depression inventory,26 or remission. Acceptability was defined as early treatment discontinuation (dropout) or non-completion of the study. Tolerability was defined as patients experiencing reported adverse drug effects including death, suicidality, and effects relating to major organ systems (cardiovascular system (eg, arrhythmias, QTc prolongation); central nervous system (eg, headache, anxiety, insomnia, hypersomnia); dermatological; endocrine system; ear; eye; gastrointestinal; genital urinary and reproductive; haematological; musculoskeletal; respiratory; and other non-categorical adverse drug effects).
Review design and setting
Reviews assessing dose-response effects for oral SSRI use in human adults for the treatment of moderate to severe depression were included. Data from the following study designs were included: pooled data, systematic literature, narrative, meta-analysis, meta-regression, or network meta-analysis. Data from primary and secondary care were included—although currently most antidepressants are prescribed in primary care to treat depression, a large proportion of the initial randomised controlled trials that inform current practice were based in secondary care inpatient or outpatient settings, not general practice. The duration of treatment was not defined in order to capture information regarding short and long term use and potential dose-response effects at different periods of depression treatment.
Information sources and literature search
We searched Embase, Medline, PsycINFO, Scopus, and Cochrane Collaboration library electronic databases. Reference lists of national and international depression treatment guidelines were searched by hand to identify previous reviews.24–28 Reference lists of editorials, commentaries, and letters identified from the electronic database searches were also searched for previous reviews. We searched for reviews or meta-analysis for all licensed SSRIs (citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, and sertraline) as monotherapy for the treatment of major depressive disorder. Key search terms included “systematic review,” “meta-analysis,” “dose-response relationship,” “dose-response,” “antidepressant$,” “antidepressive agent$,” “citalopram,” “escitalopram,” “fluoxetine,” “fluvoxamine,” “paroxetine,” “sertraline,” “serotonin uptake inhibitor$,” “serotonin reuptake inhibitor$,” “SSRI,” “depression,” “depressive disorder,” “depressive disorder major,” “unipolar depression,” “major depressive disorder,” and “human” (online supplemental file 1).
Studies on fluoxetine were first published in the mid-1970s; the SSRI that has been available on the market for the longest period.49 Therefore, 1975 was used as the start date until the end of December 2021. Reviews were limited to English language.
Literature inclusion process and data extraction
Article titles and abstracts were screened for inclusion. Subsequently, potentially relevant full text articles from the literature search were then screened for inclusion by a structured process and standard terms supporting inclusion and exclusion. Studies that did not meet the criteria outlined above were excluded.
We extracted the following data for each review article using a standardised data collection form specifically designed and tested for this systematic review: review characteristics (eg, lead author, type of review, protocol driven review, patient level data or not, type of depression being treated, review setting in primary or secondary care), antidepressant and comparator information (eg, SSRI used, fixed or flexible dose study, placebo controlled, dose standardisation technique, treatment duration), and dose-response effects (eg, efficacy, dropouts, and adverse drug effects).
Risk-of-bias assessment
Each review article was assessed according to the ROBIS (risk of bias in systematic reviews) tool,50 in line with Cochrane recommendations.32 Reviews were assessed by CFJ using ROBIS and checked by SM. The ROBIS tool has been specifically developed and designed to assess reviews within healthcare settings, and has three phases: assessment of relevance, identification of concerns with the review process, and judgment of risk of bias. The second phase covers four domains: study eligibility criteria, identification and selection of studies, data collection and study appraisal, and synthesis of findings. The third phase assesses overall risk of bias (low, high, unclear) from interpretation of review findings, and considers limitations identified in any of the domains in the second phase.50
No consensus exists on how best to assess and deal with overlap (ie, duplication), where primary studies are included more than once across two or more reviews that might bias findings; although a range of methods have been applied (such as only including meta-analysis or reviews assessed as being at low risk of bias), these could lead to loss of information.51–53 In order to avoid loss of information, and to demonstrate the diversity of reviews that met inclusion criteria, we conducted a subanalysis assessing the corrected covered area (CCA) for reviews assessed as being at low risk of bias. A citation matrix and pairwise CCA were calculated and tabulated according to Cochrane guidance.53 54 Grading was applied, as previously defined by Pieper et al.53 Similarly, no consensus exists regarding sensitivity analysis and how best assess sensitivity of findings; therefore, findings from the CCA analysis were analysed to identify discordant review findings and assess differences.52
No consensus exists on how best to assess and present data on the quality of primary studies.52 Therefore, for reviews assessed as being at lower risk of bias, we determined the methodological quality of the primary studies using the review authors’ original assessment of risk of bias by domains. Primary studies were classified as having low risk of bias if none of the domains was rated as high risk of bias and three or less were rated as unclear risk; they were classified as having moderate risk of bias if one or none was rated as high risk of bias but four or more were rated as unclear risk; and all other cases were assumed to relate to a high risk of bias.55 We then identified overall primary study quality, across the reviews at low risk of bias, by applying the most frequent quality assessment rating (eg, for three reviews rating a primary study as high, high, and low risk of bias, the study was recorded as high); for primary studies included in two reviews that did not agree on rating, the lower assessment rating was applied (eg, with a high and moderate risk of bias, the study was recorded as high).
Data analysis, synthesis, and ethics
In view of the heterogeneity of primary reviews, owing mainly to methodological diversity (ie, narrative, meta-analysis, network meta-analysis, meta-regression), it was considered appropriate to apply a meta-narrative synthesis approach.34 Tables were used to summarise the population, interventions, and outcomes of interest.
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research, owing to the lack of resources to enable such involvement.
Results
Dose-response effects of selective serotonin reuptake inhibitors
A total of 9138 records were identified from electronic search, hand searching reference lists, and grey literature. We assessed 387 full text reports for eligibility, and 42 reviews based on published and unpublished reviews matched the inclusion criteria: 25 assessed SSRI efficacy, adverse drug effects, and dropouts; 14 assessed SSRI efficacy only; and three assessed adverse drugs effects and dropouts only (figure 1). The year of publication ranged from 1988 to 2021. A range of review methods were used: 60% (n=25) were meta-analyses (14 systematic reviews, seven non-systematic reviews, and four reviews using pooled study data) and 40% (n=17) were narrative reviews (including three that reported to have systematically identified primary studies, and eight that had included a mix of primary and secondary studies (meta-analysis and/or narrative reviews); table 2 and online supplemental table S2).
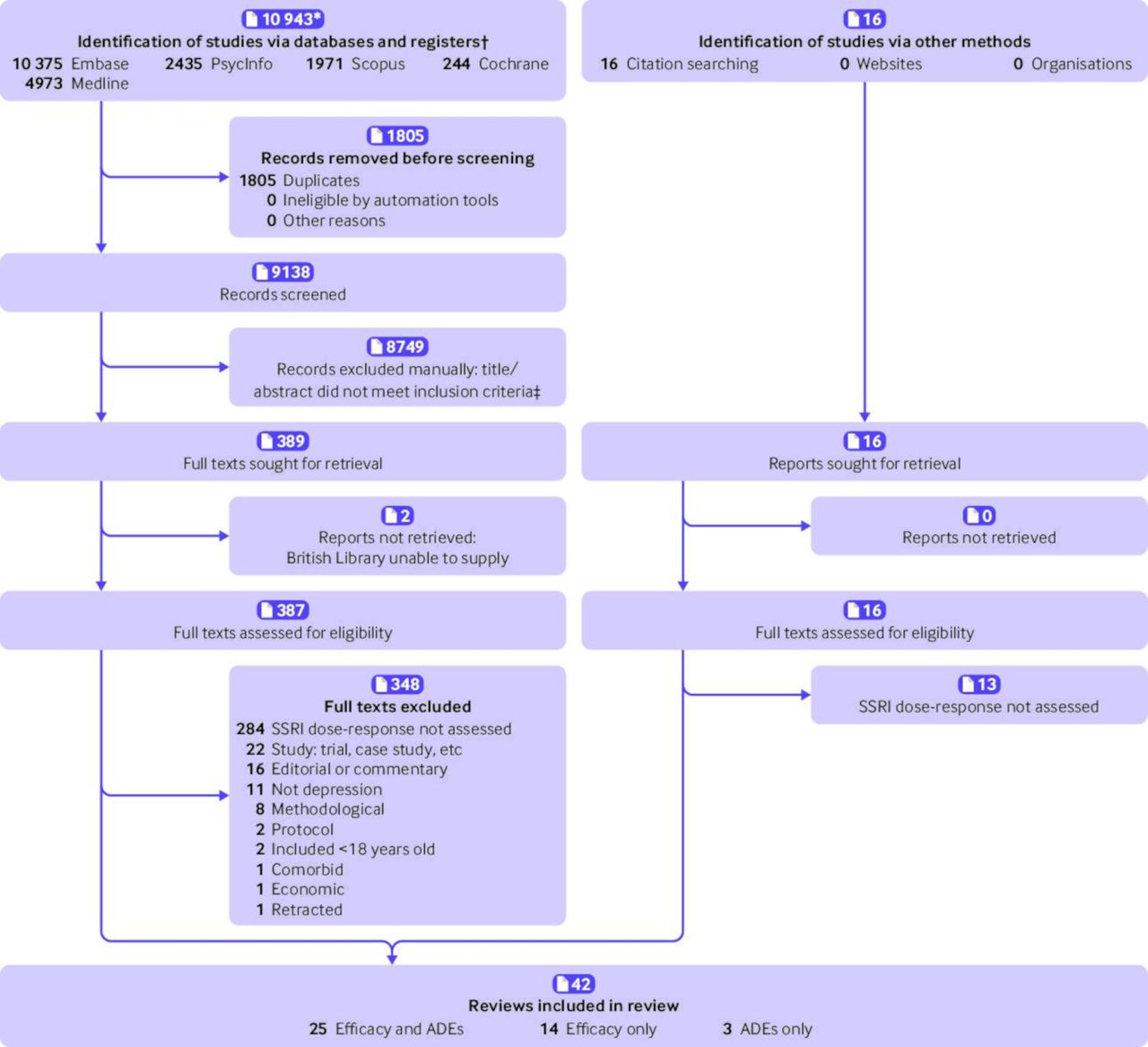
Review identification, inclusion, and exclusion. *Total records identified include combined records from Embase, Medline, and PsychInfo (n=8728), plus those from Scopus and Cochrane. †Number of records listed are those identified from each database (rather than the total number across all databases). ‡No automated tools used, as per PRISMA 2020 guideline. SSRI=selective serotonin reuptake inhibitors; ADE=adverse drug effect
Efficacy, dropouts (acceptability), and adverse effects (tolerability) of eligible reviews investigating dose-response effects of selective serotonin reuptake inhibitor monotherapy for the treatment of depression
Of the 42 reviews identified, 83% (n=35) included data from studies for 12 weeks or less (the acute phase of depression treatment), whereas five did not define the treatment period and two lacked greater detail. Four reviews considered the continuation phase and relapse prevention, but did not report on dose-response effects during the continuation phase.56–59 The care setting also varied; 17% (n=7) of reviews reported to have included data from studies conducted in primary care (general practice or outpatient clinics), 26% (n=11) included data from studies conducted in both primary and secondary care, whereas 57% (n=24) did not define the care setting.
Efficacy
The majority of reviews, 93% (n=39), assessed SSRI dose-response effects for the treatment of depression (table 2). Most reviews (n=26) indicated that the SSRI class of antidepressant demonstrated flat dose-response effects for the acute phase of treatment of depression; higher than standard daily doses did not provide greater efficacy.13 20 56 57 59–80 A minority (n=8) demonstrated that higher doses were more efficacious,18 19 23 81–85 while others (n=3) showed mixed effects,21 86 87 or remained ambiguous.22 58
At an individual SSRI level, most reviews also demonstrated flat dose-response effects for efficacy; standard daily starting doses were the optimal doses: 20 mg citalopram, 10 mg escitalopram, 20 mg fluoxetine, 20 mg paroxetine, and 50 mg sertraline (table 3).13 20 23 56 57 59–64 67 68 70–73 75–80 82 86 A minority of reviews however, indicated that some SSRIs did have linear dose-response effects with higher doses being more effective, for example, escitalopram87; citalopram (eg, up to 30 mg/day18 23 81 85 86); fluoxetine82 87; fluvoxamine13; paroxetine18 81; and sertraline.18 Other reviews indicated mixed curvy linear efficacy with increasing doses for fluvoxamine86 and sertraline.23 81 All curvy linear efficacy responses were characterised by having an initial increase, a peak, and and then a decline in efficacy with increasing dose.
Efficacy dose-response effects by individual selective serotonin reuptake inhibitor*
Blood plasma concentrations of fluoxetine, fluvoxamine, and paroxetine were assessed in association with response rates to depression treatment. We found no correlation between blood plasma concentrations and individual responses to treatment, regardless of the severity of depression.70 72
Six reviews compared the efficacy of fixed daily doses with flexible dose regimens for individuals not achieving satisfactory symptom resolution or remission (two narrative reviews73 80 and four meta-analyses62 63 66 87). All reviews demonstrated that use of flexible dose titration for these individuals did not provide greater efficacy.
Acceptability and tolerability
Of the 42 reviews, 28 (67%) assessed and reported the dose-response effects related to acceptability (early treatment discontinuation—dropouts) and tolerability (reported adverse drug effects). All reviews demonstrated that dropouts and adverse drug effects increased with increasing dose (table 2).
At a class and individual SSRI level, the following adverse drug effects were associated with (but not limited to) dose-response effects: nausea, sexual dysfunction, fatigue, anxiety, and insomnia.13 20–23 57 58 60 63 68 70–73 75 77 82 85 86 88–90 A network meta-analysis identified escitalopram as potentially providing the optimal balance between efficacy and tolerability.87 However, this study considered that escitalopram doses up to 27 mg/day might be more effective, and all SSRIs demonstrated a poor risk-benefit ratio for older adults (age >70 years old) owing to adverse effects exceeding potential efficacy.
In the six reviews comparing flexible upward dose titration with maintenance dose for individuals not achieving satisfactory symptom resolution or remission, researchers also demonstrated that higher doses were associated with poorer acceptability and tolerability.62 63 66 73 80 87
Risk of bias
The assessment revealed that the minority (12%, n=5) of reviews were at low risk of bias (table 2, figure 2 and online supplemental table S3).23 60–63 Four reviews demonstrated a flat dose-response effect for efficacy, and a positive dose-response effect for adverse drug effects and dropouts for all SSRIs.60–63 One review, however, indicated that citalopram demonstrated efficacy dose-response to 30 mg/day, and sertraline showed curvy-linear effects peaking at about 75 mg/day.23 Thirteen (31%) reviews were assessed as having an unclear risk of bias, whereas the majority (57%) had a high risk of bias that was mainly associated with a range of methodological issues.

ROBIS (risk of bias in systematic reviews) assessment of all 42 reviews meeting inclusion criteria. First four columns relate to judgments; last column relates to overall rating for risk of bias
Overlap assessment of primary studies across the five reviews at low risk of bias was very high, with a CCA of 26%.23 60–63 Pairwise overlap assessment indicated that one review demonstrated slight overlap (≤5%), whereas the reviews by Cheng et al 2020 and Furukawa et al 2019 and 2020 demonstrated high to very high overlap (figure 3). However, Furukawa et al (2019)23 found that the optimal daily dose ranged between 20 mg and 40 mg fluoxetine equivalents, and citalopram up to 30 mg daily, which was at odds with the majority of reviews showing that 20 mg fluoxetine equivalents were optimal doses at a class and individual drug level.60–63

{kind=link}
{kind=link}
{kind=link}
Corrected covered area pairwise matrix of primary studies citations.23 60–63 Pairwise analysis of review citations assessed as being at low risk of bias. Overlap categorisation: slight (0-5%; white), moderate (6-10%), high (11-15%; yellow), very high (>15%; red)
Finally, of the 160 primary studies included in the five reviews, overall risk of bias was rated as low in 34 (21%) studies, moderate in 120 (75%), and high in six (4%) (online supplemental table S4). The majority of primary studies include participants aged ≥18 to ≤65 years, with an average age of about 40 years. Six (4%) primary studies assessed antidepressant effects for older adults (age >65 years), limiting the assessment of dose-response effects for this population. Eleven (7%) of the primary studies were identified as inlcuding patients with mild depression as defined in current guidelines (eg, Hamilton Depression 17 rating scale score <17).26 However, after exclusion of the reviews that included people with mild depression,23 60 61 63 lower doses continued to show non-inferiority to higher doses.62
Critical evaluation of previous reviews
Most reviews indicated that SSRIs had a flat dose-response effect for efficacy, and poorer acceptability and tolerability with higher doses for the treatment of depression. However, a range of methodological difficulties remain, which could explain some of the conflicting findings. Firstly, only a few reviews exclusively included or reported the effects of fixed dose studies,13 20 22 23 57 66 68 71 73–75 79 while the majority included flexible dose studies. A weakness of reviews including flexible dose studies is that it requires clinicians to make a judgment early in treatment to increase the dose, which creates additional placebo effects that might be associated with the dose change, sometimes after several weeks of treatment.80 This intervention could make drug response difficult or impossible to distinguish from spontaneous remission, because 50% of patients with clinical depression spontaneously remit within 12 weeks.91 Furthermore, increasing doses could fit with patient’s expectations regarding dose effects,31 leading patients to receive higher than necessary doses, and potentially influencing the results of reviews using patient level data from flexible dose studies.18 56 75 Flexible dose studies might also select dose tolerant patients who are able to complete these studies,92 limiting generalisability and applicability to the wider population, and exposing patients to avoidable adverse drug effects. Newer reviews however, have compared the differences in effects between fixed and flexible dose studies, and report that no identifiable differences in efficacy between the groups, but that patients experience more adverse drug effects and dropouts with higher doses in both groups.62 63 87
Secondly, dose standardisation and drug grouping techniques (eg, imipramine dose equivalents and fluoxetine dose equivalents) standardise individual drugs from different classes with different doses, or dose ranges, against the tricyclic antidepressant imipramine or the SSRI fluoxetine.19 21 23 61 63 65 81 84 87 Although standardisation might seem to have benefits, use of such grouping methods inadvertently oversimplifies antidepressant pharmacology, potentially missing differences between and within drug classes. It does not take account of, or even consider that, these grouping might be inappropriate. Unlike SSRIs that are highly specific for inhibiting serotonin transporter reuptake and increasing presynaptic serotonin levels, tricyclic antidepressants, SNRIs, and other non-SSRI antidepressants have mixed serotonin and non-serotonin (norepinephrine, dopamine, melatonin, muscarinic) effects that influence their dose-response efficacy and their adverse drug effect profiles.10–12 14 93 Therefore, grouping drugs with different dose-response characteristics might provide questionable findings. Nonetheless, a few of these reviews have also presented their findings for individual SSRIs that aid clarity and could help to better inform practitioners.23 61 63 81 87
Another difficulty with imipramine dose equivalents is that researchers have used irregular dose groupings: imipramine doses of <100, 100-199, 200-250, and >250 mg/day.19 21 Introducing these groupings reduces sensitivity to detect dose-response differences, and gives greater weight to those patients that can tolerate higher doses. Imipramine dose equivalents are also based on arbitrary SSRI doses that cannot routinely be prescribed in clinical practice (eg, 45 mg citalopram, 125 mg sertraline, and 33.3 mg fluoxetine). However, other dose standardisation techniques have different limitations; for example, Braun et al compared non-equivalent low (potentially subtherapeutic) SSRI daily doses with standardised doses of the same compound (eg, ≤10 mg citalopram (equivalent to 5 mg escitalopram) v ≤9 mg escitalopram (equivalent to 18 mg citalopram)).60 Citalopram is a racemic 50:50 mixture of active S-enantiomer (escitalopram) and inactive R-enantiomer, such that 2 mg of citalopram contains 1 mg of S-citalopram (escitalopram) and 1 mg of R-citalopram.94–96 Conversely, Braun et al also categorised a wide range of doses as high in their study, which could have affected their findings—for example, ≥40 mg citalopram with ≥80 mg fluoxetine.60 But other systematic reviews have focused on individual SSRIs, using the actual drug dose—therefore, removing interclass and intraclass variations.13 18 20 56–59 61 67 71–76 78–80 85 86 88
Few reviews focus on primary care (ie, general/family practice and outpatients).67 68 71 72 83 89 While some reviews combine primary and secondary care inpatient studies,23 59 63 65 69 73 75 76 81 82 86 87 most lack clarity regarding the study settings.13 18–22 56–58 60 62 64 66 70 74 77–80 84 85 88 90 Therefore, the inclusion of inpatient studies could limit the generalisability of their findings to wider primary care populations, as demonstrated by Cheng et al.61 Other methodological limitations include: inclusion of mild depression studies23 61 63 74 81; non-placebo controlled studies22 23 81 82; narrative reviews that might lack a systematic approach20 57–59 64 68 70 71 73 77 79 80 85 86 88 89; use of data on file, which misses search strategies and misses references, preventing others from replicating the review56 66 75 76 81; assessing and reporting on efficacy but not on adverse effects or dropout rates18 20 56 59 61 64–67 69 74 76 78–81 83; and assessing response without reporting remission effects. However, even after considering the potential limitations of previous reviews, this systematic review of reviews and meta-narrative synthesis shows an overall consensus that SSRIs demonstrate a flat dose-response effect for efficacy, and poorer acceptability and tolerability as SSRI doses are increased for the treatment of depression.
Discussion
Principal findings
Ambiguity regarding SSRI dose-response and optimal dosing for the treatment of depression has been a major challenge for prescribers, and for guideline developers in Europe, North America, and Australasia. This systematic review of reviews indicates that all individual SSRIs, except for fluvoxamine, demonstrate a ceiling effect for efficacy, and poorer acceptability and tolerability as SSRI doses were increased during the acute phase (up to 12 weeks) of depression treatment for adults. Dose-response efficacy, however, remains unclear for fluvoxamine.
The prescribing of higher than standard daily SSRI doses was associated with higher rates of early treatment discontinuation (poorer acceptability) and a higher incidence of adverse drug effects (poorer tolerability) such as, but not limited to, nausea, sexual dysfunction, anxiety, and insomnia. Comparison of fixed standard daily dose and flexible dose regimens for individuals not achieving satisfactory symptom resolution or remission demonstrated that dose titration above standard daily doses did not provide greater efficacy, but was associated with poorer acceptability and tolerability.
Strengths and weaknesses of the study
A major strength of this review was the inclusion and assessment of a range of meta-analyses and narrative reviews that met the inclusion criteria, and demonstrated the breadth and depth of review literature assessing SSRI dose-response effects. To our knowledge, this is the first review of reviews to investigate SSRI drug-response effects.
Although the literature search aimed to be as comprehensive as possible and included a range of reviews using different methodologies, it is possible, as with all systematic reviews, that an important review could have been missed. However, searching a range of key electronic databases and hand searching reference lists from guidelines and other sources helped to reduce the risk of missing relevant reviews. Inclusion of reviews in languages other than English could have been beneficial, but funding was not available for this inclusion. While inclusion of reviews only in the English language might be considered to limit generalisability of findings, the majority of reviews that were assessed as being at low risk of bias included non-English language primary studies, therefore overcoming language limitations.23 60–63
Other potential limitations were that data from individual published and unpublished randomised controlled studies might not have been included in the initial review. The reporting quality of many of the older reviews was assessed as being poor with a high risk of bias, mainly because of data collection and study appraisal issues (online supplemental table S3). Overlap of primary studies within the reviews might be considered a limitation, and while no clear guidelines exist on how best to resolve it,51 the analysis of reviews at low risk of bias indicated a high to very high overlap. In 2019, Furukawa et al found that the SSRI class and citalopram dose-response between 20 mg and 40 mg per day,23 being at odds with reviews assessing similar datasets and those with no overlap.61–63 On the other hand, the lack of primary studies assessing dose-response effects for older adults was a clear limitation, and warrants further investigation. Similarly the quality of primary studies is a potential limitation, but most were considered to be at low to moderate risk of bias. Furthermore, a high degree of heterogeneity existed between the 42 reviews owing to methodological diversity and the progressive development of systematic review methodologies since 1988. Despite this, the review of reviews found a general consensus between older and newer reviews that SSRIs demonstrated flat dose-response effects for the treatment of depression, and larger doses were associated with more adverse drug effects, even when reviews assessed as having a higher risk of bias were excluded. Owing to similar results being observed across and within the reviews, including data from primary and secondary care settings, the findings appear to be generalisable to routine primary and secondary care practice, and are considered as being relatively robust.
Comparison with other studies
As already acknowledged, to our knowledge, this is the first review of reviews to investigate SSRI dose-response effects. However, the findings are congruent with previous studies indicating that serotonin reuptake receptors are highly saturated when standard SSRI doses are given; exerting a ceiling effect for efficacy at standard daily doses (20 mg citalopram, fluoxetine, paroxetine; 50 mg sertraline; and 10 mg escitalopram), providing optimal receptor occupancy and serotonin effects.10 By contrast, tricyclic antidepressants, SNRI antidepressants, and other non-SSRI antidepressants demonstrate multiple receptor effects (serotonin, norepinephrine, dopamine) with increasing doses that influence their efficacy.11 12
At an individual SSRI level, reviews carried out in the early 1990s indicated that citalopram, fluoxetine, paroxetine, and sertraline showed flat dose-response effects for efficacy with standard daily doses providing optimal efficacy.56 57 59 68 72 75 Guidelines from the British Association of Psychopharmacology and Australian and New Zealand Royal College of Psychiatry have highlighted SSRI dose limitations for the treatment of depression for several years.24 25 The recently published guidelines from the National Institute for Health and Care Excellence (NICE) advise increasing doses as one of several treatment options, and now better acknowledge dose limitations in general. However, NICE does not distinguish between drug classes,97 and the US and Canadian guidelines fail to highlight dose limitations.27 28
Meaning of the study
The findings present several challenges for practice and policy makers. Firstly, these results suggest that increasing the dose might not be more effective for the treatment of depression.24 26–28 By contrast, higher SSRI doses might be more effective for some anxiety disorders, but not others.98 99 Therefore, future local and national depression guidelines, and standard texts such as the British National Formulary, should clearly state the difference in dose-response between drug classes, and where possible between individual antidepressants, and clearly state the need to exercise caution with higher SSRI doses.
Secondly, prescribers might find this study’s findings of use when discussing and balancing drug related benefits and harms with patients and colleagues who might believe that higher doses would be more effective than standard daily doses.31 100 The findings could help with planning follow-up reviews for patients, because previous meta-analyses have indicated that the greatest response to SSRIs occurs within the first two weeks of treatment.101 102 One meta-analysis identified in this review indicated that 50% of response effect was achieved by four weeks of treatment.61 Therefore, assessing response at four weeks could help to appropriately optimise treatment more quickly; reducing the average 8-12 week delay until antidepressants are switched.100 103
Thirdly, higher than routine daily doses could expose patients to avoidable adverse drug effects, harms, and risks, such as a greater risk of QTc prolongation, falls, hip fracture, emotional blunting, cognitive dysfunction, and drug induced anxiety and insomnia.104–108 Some of these adverse drug effects might be mistaken for depressive symptoms that could require more follow-up appointments, treatment with a higher SSRI dose, or the coprescription of sedating antidepressants, benzodiazepines and/or antipsychotic drugs, resulting in unnecessary polypharmacy.109–111 Furthermore, the use of higher SSRI doses could be associated with a greater risk of withdrawal symptoms that might result in prolonged treatment.112
Finally, as SSRIs account for 43-76% of antidepressant prescriptions in North America, Europe, and Australasia,1 2 4 6 7 and account for more than 65% of antidepressant defined daily doses prescribed in Scotland,4 the use of higher daily doses and a lack of prescriber awareness regarding dose limitations could be contributing to inappropriate antidepressant use and to the current growth in prescribing.5 7–9 100
Future research should consider examining dose-response effects with longer term SSRI use, which has increased over the years and is associated with the prescribing of higher SSRI doses.5 7–9 113 114 The following research questions could also be considered: do placebo controlled trials demonstrate that higher SSRI doses are more effective for people experiencing loss of efficacy (tachyphylaxis) with long term treatment115; do neuroprogressive changes in depression affect drug response, and vice versa116 117; do acute on chronic depressive episodes require higher doses; does increasing or reducing doses provide non-drug effects118 119; and how these factors interact to affect drug response.120 A greater focus is also needed to assess and report the achievement of remission that could help to improve patients’ long term outcomes. Qualitative studies should be considered to provide insight into patients’ lived experiences and expectations regarding antidepressant doses and drug limitations; as well as being used to help contextualise findings from potential quantitative studies. Lastly, a better understanding of possible dose related SSRI effects associated with withdrawals (discontinuation symptoms) could enable prescribers to support patients to discontinue treatment, as highlighted in petitions to the UK parliaments and recommendations from Public Health England and the Scottish government.1 121–124
Conclusion
Standard daily SSRI doses could provide a favourable balance between efficacy, acceptability, and tolerability for the acute phase (up to 12 weeks) treatment of depression in adults. Higher daily doses were associated with higher rates of early treatment discontinuation (poorer acceptability) and a higher incidence of adverse drug effects (poorer tolerability) such as, but not limited to, nausea, sexual dysfunction, fatigue, anxiety, and insomnia. We also would encourage patients to talk to their prescriber or community pharmacist if they experience adverse effects or have any concerns about their drug treatment.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics approval
This systematic review did not require ethical approval.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CFJ identified the inconsistencies in the literature, identified the scope and rationale for the review, and conceptualised the systematic review. CFJ and SM designed the protocol and analysed data. All coauthors (CFJ, MM, BW, ND, and SM) have substantially contributed to the interpretation of the data, writing of this article, provided critical revision, and gave final approval of the published version. CFJ is the study guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. Transparency: The lead author (the guarantor) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Funding This project is funded by educational bursaries from NHS Greater Glasgow and Clyde and the Pharmacy and Prescribing Support Unit Endowment fund. This work is independent of the funders and does not necessarily represent their view.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from the NHS Greater Glasgow and Clyde and the Pharmacy and Prescribing Support Unit Endowment fund for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.