Article Text

Abstract
Throughout human history, infection has been the leading cause of morbidity and mortality, with pain being one of the cardinal warning signs. However, in a substantial percentage of cases, pain can persist after resolution of acute illness, manifesting as neuropathic, nociplastic (eg, fibromyalgia, irritable bowel syndrome), or nociceptive pain. Mechanisms by which acute infectious pain becomes chronic are variable and can include immunological phenomena (eg, bystander activation, molecular mimicry), direct microbe invasion, central sensitization from physical or psychological triggers, and complications from treatment. Microbes resulting in a high incidence of chronic pain include bacteria such as the Borrelia species and Mycobacterium leprae, as well as viruses such as HIV, SARS-CoV-2 and herpeses. Emerging evidence also supports an infectious cause in a subset of patients with discogenic low back pain and inflammatory bowel disease. Although antimicrobial treatment might have a role in treating chronic pain states that involve active infectious inflammatory processes, their use in chronic pain conditions resulting from autoimmune mechanisms, central sensitization and irrevocable tissue (eg, arthropathy, vasculitis) or nerve injury, are likely to cause more harm than benefit. This review focuses on the relation between infection and chronic pain, with an emphasis on common viral and bacterial causes.
- Allergy and immunology
- COVID-19
- Pain
- Infectious disease medicine
- Respiratory tract infections
- Hiv
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Pain is the leading cause of years lost to disability worldwide, and the most common reason for seeking healthcare.1 2 Teleologically, pain serves as an existential protective mechanism against internal and external stimuli that threaten an organism, with evidence that even the most primitive organisms experience nociception, including fish and invertebrates.3
Throughout history, infectious diseases have exacted the greatest toll on humankind in terms of morbidity and mortality, and dolor (pain) is a cardinal sign of infection.4 Although our bodies eradicate most infections, a substantial percentage will persist in a sublethal or lethal form because of failure in detection or treatment (table 1). In other individuals, an infection could resolve but trigger an enduring immune response that results in chronic pain, which can occur in 10-33% of cases of nociplastic and post-infectious pain syndromes, or serve as a psychological stressor that initiates or exacerbates chronic pain.5–8 The inextricable link between chronic pain and infection is illustrated in a recent study evaluating nearly 2 million patients with covid-19, which found chronic pain to be the most common lingering complaint at least 30 days after diagnosis, affecting 5.1% of the 23% of patients with so-called long haul symptoms.9 To date, a comprehensive analysis on chronic pain syndromes after infection has yet to be undertaken.
Pain syndromes commonly associated with infectious causes115 189–191
Sources and selection criteria
Between September 2021 and January 2022, we searched the following databases for articles pertaining to chronic pain and infection: PubMed, Embase, OVID, and Google Scholar, without language or date restrictions. We cross referenced the major search terms "chronic pain," "pain," "vaccine," "antibiotic," "antiviral," "mechanism," "infection," and "complication" with various iterations and subcategories of these keywords to correspond with various pathogens, drug treatments, mechanisms (eg, "bystander activation"), and chronic pain conditions. We prioritized peer reviewed systematic reviews and large clinical trials, but included narrative reviews, case series, and retrospective studies as indicated. In addition to primary sources, we searched reference lists of retrieved articles.
Mechanisms
Acute pain
Infection can cause pain via numerous mechanisms. Acutely, pain is a core symptom of infection, and could result directly from somatic (eg, septic arthritis) or visceral (eg, appendicitis) tissue invasion, or nerve injury (eg, acute herpes zoster neuritis) and the accompanying inflammatory process.
Chronic pain
Molecular mimicry and other immune mechanisms
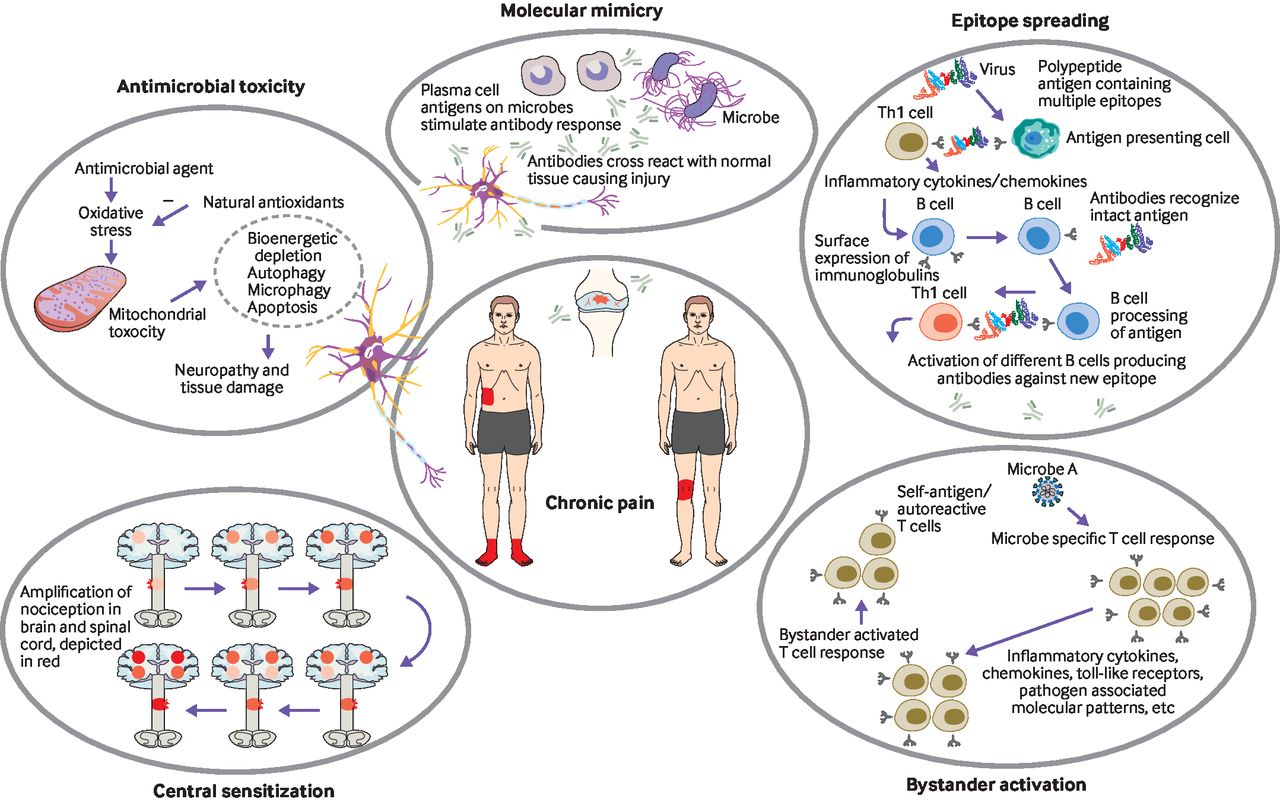
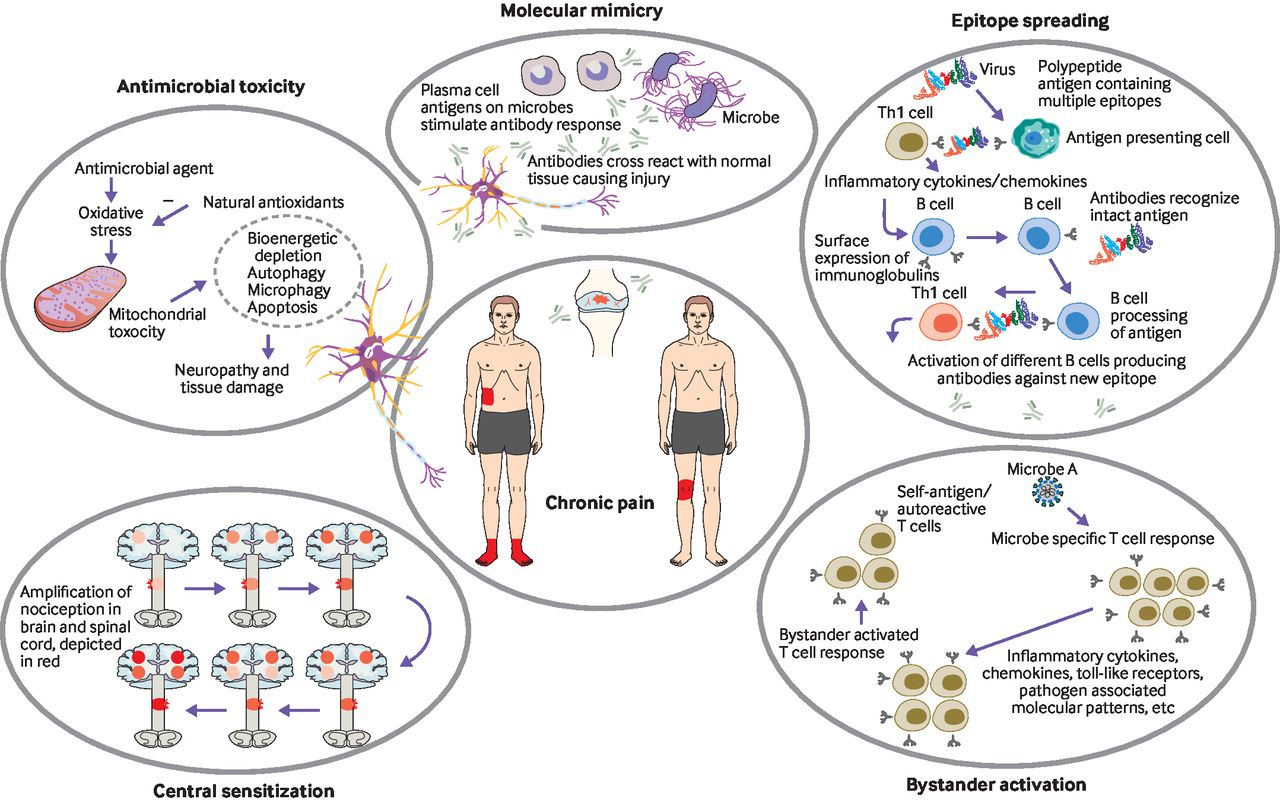
Figure 1 shows the various mechanisms by which chronic pain can occur after infection. Inflammation after infection might cause an abnormal immune response that triggers acute and chronic neuropathic, nociceptive, or nociplastic pain. In Guillain-Barré syndrome, immunoglobulin G induced, painful peripheral neuropathy affects between 55% and 89% of individuals, with two thirds of patients experiencing a viral (eg, Epstein-Barr virus, Zika virus) or bacterial (eg, Campylobacter jejuni) infection within the preceding six weeks.10–12 The precise mechanisms for axonopathy are unclear, but evidence points to mimicry of axolemmal surface molecules (gangliosides) by microbial antigens (lipopolysaccharides), leading to an antibody mediated attack on the nerve axolemma. Other immune related painful conditions in which molecular mimicry is postulated to have a role include multiple sclerosis, reactive arthritis, inflammatory bowel disease, and Lyme disease. Similarly, infection could trigger autoimmune related pain via epitope spreading and bystander activation. In epitope spreading (also known as antigen spreading), endogenous epitopes develop secondary to the release of self-antigens during inflammation.13 Bystander activation is characterized by autoreactive B and T cells that are activated in an antigen independent manner.14
{kind=link}
Mechanisms of chronic pain after infection
Viral gene products or remnants
Preclinical studies have shown that products produced by viral infections could enhance pain sensitivity. In rodents, elevated levels of the inflammatory enzyme indoleamine-2,3-dioxygenase heighten pain sensitivity, which returns to normal as the infection clears, or remains elevated with persistent infection (eg, murine leukemia retrovirus, an analogue of human immunodeficiency virus (HIV)-1).15 These findings are consistent with studies demonstrating increased pain sensitivity in people living with HIV with detectable viral loads compared with controls without HIV or with HIV without detectable virus loads.16 Persistent infection and resultant peripheral and central sensitization might be particularly common with herpes viruses (eg, Epstein-Barr virus, cytomegalovirus, human herpes viruses 6 and 7), which can remain dormant for years and are a common antecedent for myalgic encephalitis or chronic fatigue syndrome, which is frequently characterized by diffuse chronic pain. Retroviruses such as HIV and human T cell lymphotropic virus type 1, which integrate into the genome, might also contribute to persistent symptoms and sensitization.17–19 Diffuse, chronic pain is a hallmark of most diagnostic criteria for myalgic encephalitis or chronic fatigue syndrome, and active HIV infection is associated with myriad neuropathic, nociceptive, and nociplastic pain symptoms, suggesting viral induced central sensitization.20 21 Similarly, viral remnants such as mRNA or proteins, or even subdetectable levels of virus, could promote a persistent immune response which results in pain and other symptoms typically associated with acute infections.22
Treatment associated chronic pain
Vaccine reactions—Vaccines are designed to induce an immune response. After entering the body, antigen derived (pathogen associated) and host derived (damage associated) molecular patterns bind to pattern recognition receptors such as toll-like receptors found on circulating immune and stromal cells. This event results in transcription of target genes leading to the synthesis and release of inflammatory cytokines (eg, interleukin 1, interleukin 6, tumor necrosis factor alpha). An immunologic cascade is initiated, mimicking an attenuated response to infection, leading to phagocytosis, release of acute phase reactants, and further release of inflammatory mediators including chemokines and cytokines, complements, and leukocytes.23 The local production of inflammatory mediators can lead to site specific pain, while systemic circulation can result in diffuse symptoms that include headache, myalgias, arthralgias, and rarely neurological symptoms.23 24 Although very rare, long term sequelae of certain vaccinations have been reported including persistent localized pain at the inoculation site and Guillain-Barré syndrome.25 26
Antimicrobial and surgical treatment—antibiotics and antiviral treatments could be associated with chronic pain conditions such as peripheral neuropathy, usually in dose dependent or time dependent fashions. An association between antibiotic use and peripheral neuropathy has also been found for other drugs (table 2). Mechanisms of antibiotic induced neuropathy might include axonal toxicity, demyelination, and conduction blockage.27
Antimicrobial drug treatments associated with neuropathy and other pain conditions192–194
Antiviral drug treatments such as nucleoside analogue reverse transcriptase inhibitors and interferon α might be prescribed for a prolonged time for infections with HIV and hepatitis, increasing the likelihood of toxicity. Nucleoside reverse transcriptase inhibitors such as didanosine and stavudine could cause myopathy characterized by muscle wasting, myalgia, weakness, and elevation of creatine kinase, as well as a dose dependent neuropathy that is painful and axonal in nature.28 Other pain conditions associated with antimicrobial drug treatments include vasculitis, encephalitis, arthralgia, and headache.
Surgical tissue removal and other procedures might be used to treat infection, including appendicitis, cholecystitis (>50% are secondary to infection), and necrotizing fasciitis. The prevalence of chronic pain after surgery has been cited at around 18% in children after appendectomy29 and 14% after cholecystectomy, although about 33% of patients will continue to report persistent painful symptoms after gallbladder resection.30
Common viral related neuropathic pain conditions
Neuropathic pain is defined by the International Association for the Study of Pain as "pain caused by a lesion or disease of the somatosensory nervous system,"31 and is recognized as being mechanistically distinct from nociceptive pain and nociplastic pain.32 33 Viral infections can lead to neuropathic pain by creating lesions in the peripheral or central nervous system,32 34 producing cytokines that sensitize nociceptors,35 or eliciting an immune response that attacks organ systems.12–14 Although viruses can also cause nociceptive pain (eg, arthritis), pathogenesis is varied and pathogen specific.36
Varicella zoster virus
Varicella zoster virus is responsible for chickenpox and shingles. After a primary infection, it lies dormant in a dorsal root or cranial ganglion and reactivates upon a decline in immunity. Pain can be spontaneous, paroxysmal, or evoked (eg, allodynia), and acute reactivation typically causes nociceptive (vesicular rash) and neuropathic (acute radiculitis) pain.
Postherpetic neuralgia is the most common and one of the most serious complications of acute infection with varicella zoster virus, and is defined as pain persisting more than 90 days after the onset or healing of the vesicular rash.37 Mechanisms include nerve root inflammation and ectopic discharges, peripheral sensitization, and central sensitization (eg, loss of inhibitory neurons, glial cell activation), deafferentation in the affected dermatome, and central nervous system reorganization (eg, alterations in brain metabolism, decreased grey matter, and sympatho-afferent coupling).38
Postherpetic neuralgia can eventually develop in approximately half of the individuals infected with varicella zoster virus.37 Risk factors include older age, prodromal pain, severe acute pain or rash, marked immunosuppression, and diabetes.37 39 40 Because greater acute pain and rash severity might indicate increased neural damage,40 41 treatment of varicella zoster virus and resultant acute pain could reduce the incidence of postherpetic neuralgia. Strategies have included antiviral treatment, steroids, non-steroidal anti-inflammatory drugs, neuropathic analgesics, local anesthetics, epidural steroids, and neuromodulation.42–46 However, these treatments have yielded mixed results for the prevention and treatment of postherpetic neuralgia. Vaccination is the most effective means of preventing postherpetic neuralgia, reducing risk by up to 67%, and vaccinated patients who do develop the disorder have less severe symptoms.47
Human immunodeficiency virus (HIV)
More than 30 million individuals worldwide are infected with HIV type 1 (HIV-1) or 2 (HIV-2),48 although this number is likely an underestimate because of poor access to healthcare among populations at risk.49 50 Six strains of HIV-1 account for the vast majority of infections globally.51 HIV-2 is characterized by lower transmissibility and is uncommon outside West Africa.51 52
With the development of antiretroviral treatments, the prognosis of HIV infection has markedly improved and many patients have a near-normal lifespan. However, antiretroviral drugs rarely eliminate the virus entirely. As a consequence of chronic infection, more than 50% of individuals with HIV develop chronic non-cancer associated pain.53 54 Painful peripheral neuropathy is one of the most common symptoms, with the most form having a characteristic stocking-and-glove distribution.53 55 HIV can directly cause neural damage via certain components of its viral envelope, such as glycoprotein 120, that induce axonal degeneration, inflammatory cytokine release, and increased oxidative stress.56 57 Earlier generations of antiretroviral drug treatments were associated with distal polyneuropathies,53 possibly through the upregulation of inflammatory cytokines, microglial activation, and direct neuroinflammation.58 59 Cohort studies performed before the advent of highly active antiretroviral treatments found an increased incidence and severity of polyneuropathy in individuals who are immunosuppressed and with higher viral loads, with some evidence that effective treatment might be associated with improvement in pain and other neurological symptoms.60 61
HIV infection is also associated with a greater risk of concomitant nociceptive or nociplastic pain. Patients with HIV commonly report abdominal pain, chest pain, musculoskeletal pain, and headaches,53 55 and are at higher risk of developing fibromyalgia.55 How HIV directly leads to these symptoms is unclear, but mechanisms similar to the development of neuropathic pain, including central and peripheral sensitization and psychosocial factors (eg, social isolation or stigma), are likely to be involved.55
Herpes simplex virus
The vast majority of people worldwide are infected with either herpes simplex virus type 1 (HSV-1) or 2 (HSV-2).62 Infection occurs through contact with mucosal surfaces or abraded skin. Although acute symptoms might occur,63 most individuals are asymptomatic.62 HSV-1 and HSV-2 enter sensory ganglia and establish lifelong latency.62 64 Cycles of dormancy and reactivation can occur, most commonly at mucocutaneous sites63 64 (eg, vesicular lesions at the vermilion border of the mouth, herpetic whitlow in medical and dental professionals’ fingers), often with prodromal burning, itching, or pain.63
Highly morbid painful neurological manifestations can occur. HSV-1 is associated with encephalitis63 65 and herpes keratitis, which presents with ocular pain and is one of the leading causes of infectious blindness in the world.66 Owing to its ability to establish latency in the cranial ganglia, HSV-1 might also lead to Bell’s palsy, which is sometimes characterized by pain.65 HSV-2 is associated with meningitis, ascending thoracic or lumbosacral myelitis, and lumbosacral radiculitis, and might have a synergistic relation in causing these symptoms in patients with HIV.65 HSV-1 and HSV-2 might also cause central spontaneous pain via glial activation, although the incidence and mechanism(s) are unclear.64 Antiviral drug treatments could reduce the severity and duration of symptoms, but do not eradicate the virus.
Hepatitis C virus
Hepatitis C virus is a member of the Flaviviridae family with up to 190 million individuals worldwide infected.67 68 The virus replicates up to 10 trillion copies per day without a proofreading mechanism, leading to numerous genetic variants that prevent the host’s immune system from eradicating it.67 Hepatitis C virus has the distinction of being the hepatitis virus with the most known extrahepatic manifestations,69 including arthralgia, lymphoma, type diabetes, and chronic kidney disease. Most of these conditions are independently associated with chronic pain.
The virus is also the leading cause of mixed cryoglobulinemic vasculitis, which can lead to a distal sensory or sensorimotor peripheral neuropathy that presents with painful paresthesias.69 70 Peripheral neuropathy can occur independently of cryoglobulinemia and might be more strongly associated with older age and the duration of infection with hepatitis C virus.68 71 Evidence also suggests that the virus can elevate levels of inflammatory cytokines such as interleukin 6, contributing to hyperesthesia and possibly centrally mediated pain.72
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)
Covid-19 is associated with acute pain in 20% to >60% of patients admitted to hospital, with the most common complaints being myalgia or arthralgia, headache, and sore throat (>25%); followed by chest pain, spinal pain, abdominal pain, and non-headache neurological symptoms.73–75 These symptoms can result from a combination of factors, including a hypervigilant immune response, fever, deconditioning, and direct viral invasion (arthralgia, myositis, myocarditis or chest pain).75 76 Although SARS-CoV-2 is not primarily neurotropic, the virus binds to angiotensin converting enzyme 2 receptors in the central and peripheral nervous system, and has been linked to myelitis, Guillain-Barré syndrome, and peripheral neuropathy.75 77 As with other viral mediated illness, neuropathic pain can be triggered by immune mechanisms, antiviral treatment, or direct viral invasion, and carries a higher incidence in those individuals with pre-existing risk factors (eg, diabetes).78 About 5-15% of patients admitted to hospital with covid-19 will present with abdominal pain, which might be secondary to viral binding to angiotensin converting enzyme 2 receptors in the gastrointestinal tract, lymphadenopathy, referred pain from the lungs, or visceral distension.75
In one observational study, the presence of acute pain was paradoxically found to mitigate against death and intensive care, which was attributed to the activation of neurotransmitters involved in pain modulation and distraction.74 In another case-control study, patients who experienced myalgia during acute covid-19 had a greater likelihood of having musculoskeletal pain seven months after covid-19 infection that those who did not have myalgia (odds ratio 1.41, 95% confidence interval 1.04 to 1.90).79 Several studies have found chest pain, headache, myalgias, and arthralgias to be present in over 20% of surviving patients with covid-19, 60 days after infection, with neuropathy, spinal pain, and abdominal pain reported less frequently.80 Since patients in these studies did not have measurable viral loads, the cause of these symptoms is likely immunological or a psychological triggering event.5
Common bacterial related pain conditions
Borrelia burgdorferi (Lyme disease)
Lyme disease results from infection with several Borrelia species including burgdorferi, afzelii, and garinii. Pain can appear immediately after infection (stage 1 includes, for example, localized pain and constitutional symptoms), days to weeks after infection (stage 2 includes, for example, severe headache, myalgias and arthralgias), and during a controversial stage 3, which can range from months to years after infection and has been postulated to be secondary to central sensitization.81 82
About 10-20% of patients with infection develop post-treatment Lyme disease syndrome, which entails unequivocal evidence of infection and appropriate treatment. However, in one analysis of seven observational and retrospective studies including 1902 patients in endemic areas, 50-88% of enrolled patients had no evidence of Borrelia infection.83 The cause is most likely autoimmune, with high antibodies to Borrelia burgdorferi found in some patients with reactive arthritis.83 84 Diffuse pain is a hallmark, with over 75% of individuals reporting headache, arthralgias, myalgias, neuropathic pain, and widespread pain most consistent with nociplastic pain. Similar to other nociplastic conditions, sensory hyperarousal, cognitive deficits, fatigue, and sleep dysfunction also affect most individuals with post-treatment Lyme disease syndrome.85 Although antibiotics are frequently prescribed and have been found in some studies to provide subjective benefit,85 86 the Centres for Disease Control and Prevention recommends against their routine use based on high quality trials.87
Mycobacterium leprae (leprosy)
Leprosy, also known as Hansen’s disease, causes 250 000 infections worldwide annually, with Brazil, India, and Indonesia accounting for 80% of cases.88 The bacterium responsible for leprosy, Mycobacterium leprae, is morphologically indistinguishable from Mycobacterium tuberculosis. In 1982, the World Health Organization developed a simple classification system, which categorizes patients as having paucibacillary (<5 lesions) or multibacillary (>6) leprosy, reflecting the tissue burden of the infection.89
Although sensory loss, visual impairment and disfigurement are more notorious, neuropathic pain is present in about 35% (range 11-66%) of patients. with leprosy90–92 The bacterium can enter the nervous system via endothelial cells or transmigration of infected monocytes, showing an affinity for Schwann cells. The type of neuropathic pain varies based on disease burden, with the ulnar and peroneal nerves commonly affected in paucibacillary leprosy, while advanced stages frequently result in a diffuse symmetrical polyneuropathy that often includes the facial and trigeminal nerves.92 In addition to neuropathic pain, patients with leprosy also experience nociceptive pain from tissue invasion (eg, skin, nose, testicles) and disfigurement, with lifetime prevalence rates ranging from 15 to >40%.93–95 Patients with leprosy also have disproportionate psychological distress including ostracization and stigmatization, which can exacerbate pain. Although corticosteroids are often used to treat acute neuritis from leprosy, a systematic review found no evidence for long term superiority over placebo for nerve function.93 96 Because most neuropathology in leprosy is immunological, nerve injury and neuropathic pain can occur before, during, or after antibiotic treatment.97
Group A streptococcus
In acute rheumatic fever, oropharyngeal group A streptococcus infection triggers an autoimmune response resulting in inflammation and organ damage.98 Most patients who develop rheumatic fever are aged between 5 and 15 years, with Streptococcus pyogenes being the most implicated bacterial strain. In one large database study of 1470 children, 50% of rheumatic fever hospital admissions presented with primary arthritis without carditis, 26% presented with arthritis and carditis, 24% presented with chorea, and 6.5% showed both chorea and carditis.99 Recurrences are common in rheumatic fever, especially in younger individuals. Considered by many to be a prototypical autoimmune condition, rheumatic fever can manifest as a prolonged pain syndrome that includes reactive polyarthritis, skin involvement, carditis, vasculitis, and chorea, which might result in associated neurologic symptoms including pain.98 100 About 5% of patients with untreated, group A streptococcus pharyngitis develop rheumatic fever, with early antibiotic treatment reducing the risk substantially. Prophylactic antibiotics are recommended to prevent recurrences.101
Treponema pallidum
Treponema pallidum is a spiral-shaped bacterium belonging to the phylum Spirochaetes, with subspecies that each cause a distinct disease (T pallidum subspecies endemicum, T carateum, and T pallidum subspecies pertenue cause bejel, pinta, and yaws, respectively).102 103 These subspecies are serologically and morphologically indistinguishable,103 104 spread by direct contact through dermal microabrasions or mucosal membranes, and form painful mucocutaneous ulcers. However, T pallidum subspecies pallidum, the causative agent of syphilis, is unique in being transmissible via blood and is most commonly spread through sexual contact.
Humans are the only known natural host of T pallidum subspecies pallidum.102 With the introduction of penicillin, the incidence of syphilis declined considerably in the mid-20th century.105 However, cases have steadily increased over the past 20 years in association with unsafe sexual practices (eg, unprotected sexual contact, promiscuity), with WHO estimating 12 million new cases annually across the globe.102
On infection, systemic dissemination occurs within hours, and a painless chancre—the characteristic sign of primary syphilis—appears within three weeks.102 Within three months, secondary syphilis occurs, which is characterized by a disseminated maculopapular rash and protean findings105 that can be associated with pain and discomfort, including lymphadenopathy, mucosal lesions, gastritis,106 hepatitis,107 glomerulonephritis,108 and pulmonary abscesses.109 After a latent period that is usually less than a year, tertiary syphilis begins. Neurologic manifestations are most common (eg, paresthesias, paresis, and ataxia from tabes dorsalis,102 vision loss,110 and cognitive impairments105), followed by cardiovascular complications (eg, aortic aneurysm and myocarditis) and granulomatous nodules known as gummas.102 105 Regardless of the stage of infection, penicillin is the treatment of choice,105 although even with bacterial eradication, pain could persist when organ damage is severe.
Infection and nociplastic pain
In 2016, the term "nociplastic pain" was proposed to describe pain characterized not by nerve or tissue injury, but by alterations in pain related sensory pathways leading to peripheral and central sensitization.33 Fibromyalgia is the prototypical nociplastic pain condition, but similar syndromes such as irritable bowel syndrome, bladder pain syndrome, and chronic daily headache are also considered nociplastic.
Cohort and cross-sectional studies have found that between 6% and 27% of patients with fibromyalgia report an infectious inciting event (eg, Epstein-Barr virus, Lyme disease), with up to 40% describing worsening symptoms after infection.111 112 ,113 In small case-control study, researchers contacted 22 (of 50) patients unable to return to work after severe acute respiratory syndrome (SARS); they found striking similarities to 21 female controls with fibromyalgia, and a strong overlap with chronic fatigue syndrome (CFS).114 For irritable bowel syndrome, one review reported an unweighted median in 10 studies of 10% (range 4-32%) for an infectious etiology, with the most common causes being gut pathogens (Escherichia coli, Shigella, Campylobacter, Salmonella).115 The high incidence of recurrent urinary tract infections in women and the overlap in symptoms between urinary tract infections and bladder pain syndrome (interstitial cystitis) make conclusions difficult to draw regarding an infectious cause, with clinical studies yielding mixed results.7 116 Currently, the absence of an ongoing infection is an exclusion criterion for bladder pain syndrome. For chronic daily headache (and to a lesser extent migraines), some studies of various designs report that over 20% began with an infection, although results are mixed.117–119 Some interventional studies also report the alleviation of symptoms when bacterial organisms such as Helicobacter Pylorii are eradicated.120 While rare and anecdotal, nociplastic symptoms such as diffuse body pain and persistent headaches have also been reported after vaccinations.121 122 In addition to sensitization from post-inflammatory immune reactions, region-specific causes include changes in gut microbiota and injury to enteric nerves for irritable bowel syndrome, and low grade encephalomyelitis for headaches.
Influence of postoperative infection on persistent pain after surgery
Persistent pain after surgery occurs in 10-50% of patients experiencing acute postoperative pain, with 2-10% reporting severe chronic pain.123 124 Chronic pain after surgery might result from peripheral and central pain sensitization due to inflammation, tissue damage, and nerve injury.124 125 Tissue damage and nerve injury occurring as a direct result of surgery can trigger localized and systemic inflammation in a mechanism similar to, but independent from, perioperative pathogenic infection.125 126 Patients undergoing surgery are also vulnerable to healthcare associated infections. About 7% of patients undergoing surgery have an infection during the perioperative period, resulting in substantial morbidity, mortality, and healthcare costs.127 128 Exogenous infection can compound the mechanisms of neuroinflammation and systemic inflammation that lead to chronic pain after surgery. Risk factors for persistent pain after surgery include preoperative pain, acute postoperative pain intensity and the extent of nerve and tissue damage, all of which can be amplified by infection.124 129 In addition, patients' specific immune function and inflammatory responses have been shown to correlate with surgical recovery, including postoperative pain and function.130–133
Few studies have evaluated the relation between postoperative infection and chronic pain, and few guidelines draw any explicit connection between the two. Most often, infection is considered as an alternative diagnosis for chronic pain after surgery. The International Association for the Study of Pain's classification notes that "other causes of pain such as pre-existing pain conditions or infections… have to be excluded in all cases of chronic post-traumatic and post-surgical pain."134 However, pain is a common feature of infection after surgery,135 and the presence of infection could provide sufficiently prolonged afferent stimulation to result in sensitization, a key mechanism underlying the transition from acute to chronic pain after surgery.136
A retrospective cohort analysis of nearly 12 000 adults undergoing surgery found that surgical wound infection or sepsis was the most common major postoperative complication, and was associated with a 1.53 times increased odds (95% confidence interval 1.18 to 2.05) of lingering pain after surgery, after adjusting for confounding variables.137 These findings are consistent with observational studies reporting a higher incidence of persistent pain after surgery in patients with wound complications after sternotomy138 and infection after hysterectomy.139 A recent meta-analysis of 18 prospective and retrospective gynecological and urological surgery studies found that surgical wound infection was associated with a 2.71 times (1.75 to 4.18) increased risk of persistent pain after surgery.140 Postoperative infection should therefore be considered a risk factor for persistent pain after surgery, not just an alternative diagnosis.
Risk factors for surgical site infection can be patient related (eg, age, comorbid disease, nutritional status) or procedure related (eg, complexity, surgical technique, antibiotic prophylaxis, glycemic control).128 Various guidelines provide recommendations on the prevention of infection at the surgical site, which include maintaining strict perioperative blood glucose control, adequate perioperative oxygenation, normothermia, normovolemia, and the use of various surgical related strategies to mitigate risk.128 141 Although no prospective studies have yet evaluated the association between perioperative infection prevention and persistent postsurgical pain, infection control should remain a cornerstone of perioperative care.
Controversies
Discogenic spine pain
Studies have shown that over 40% of herniated discs might be infected with bacteria, with the most common organism being the anaerobic bacterium Cutibacterium acnes.142 In one meta-analysis by Ganko et al of nine studies with various methodologies (one included cervical discs), seven studies included patients with radiculopathy or herniated disc and two included patients with disc degeneration. The researchers found a higher infection rate in degenerated discs than in non-degenerated discs (37.4% v 5.9%; odds ratio 6.077, 95% confidence interval 1.426 to 25.901).143 However, a large subsequent case-control study (n=812 total samples) that included operated cervical and lumbar discs found no difference in infection rates between symptomatic and control discs.144 A 2018 prospective study found a 32.5% infection rate in 80 patients who underwent single level discectomy for sciatica, with a positive association between infection and endplate signal changes, but not for the degree of disc degeneration.145 In another prospective study of 32 patients who underwent cervical discectomy and fusion, positive cultures were found in 25% of patients and 13.6% of discs, which was higher than the positive rate in controlled muscle biopsies (12.5%).146 In this sample, coagulase-negative Staphylococcus was the most common microbe.
Studies have sought to evaluate the efficacy of antibiotic treatment for discogenic pain. In a review by Gilligan et al, two of four observational studies and two of three randomized controlled trials (n=413) reported benefit.142 In the randomized trials, the two positive studies treated patients with Modic type 1 endplate changes for 100 days with amoxicillin-clavulanic acid and reported benefit at one year or end of treatment,147 148 while the negative study treated patients with Modic type 1 and type 2 changes with only amoxicillin for 3 months and reported no meaningful benefit at one year.149 Collectively, these results suggest that a small percentage of patients with infection-associated disc pathology might benefit from antibiotic treatment, but the heterogeneity of spine pain and lack of antibiotic penetrance could hinder results.
Inflammatory bowel disease
Inflammatory bowel disease includes Crohn’s disease, which can affect any part of the gastrointestinal tract, and ulcerative colitis, which is limited to the colon. Evidence suggests that a subset of patients with inflammatory bowel disease develops symptoms secondary to an autoimmune response that targets natural gut microbiota or fails to control invasive commensal or pathogenic organisms.150 151 In a computational analysis of a dataset from people with inflammatory bowel disease, Hassouneh et al found 34 bacterial species with concentrations at least twofold higher than that of control samples, and eight species that were less than half as abundant.152 That many of these bacteria are implicated in immune modulation and inflammation suggests the relation between microbes and immune system impairment might be bidirectional.
Numerous studies have established higher prevalence rates of organisms (such as Mycobacterium avium subspecies paratuberculosis, adherent invasive E coli, Campylobacter species, Clostridium difficile, and cytomegalovirus) in patients with inflammatory bowel disease than in control patients, with minimal differences in disease stage or type of inflammatory bowel disease. Other research, including a meta-analysis examining 58 studies with various designs, found a protective effect for Helicobacter pylori.153 One mechanism by which microbes can cause inflammatory bowel disease is via dysregulation of pattern recognition receptors, which include toll-like receptors and C type lectin receptors.154
The clinical pain presentation of inflammatory bowel disease varies according to phenotype. Abdominal pain, typically described as crampy and colicky, affects about 60% of patients, and is more common in Crohn’s disease. Crohn’s disease affects the entire gastrointestinal tract, so painful oral ulcers can occur, with a prevalence of around 30%.155 Tenesmus might occur in both Crohn’s disease and ulcerative colitis but is more common in the ulcerative colitis. Rheumatological manifestations affect up to 30% of patients with inflammatory bowel disease and are more common in Crohn’s disease, with one meta-analysis of 71 observational studies finding an average prevalence of 13% for peripheral arthritis, 10% for sacroiliitis, 3% for ankylosing spondylitis, and lower rates for enthesitis and dactylitis.156 Other painful manifestations might include cholangitis and hepatitis, ocular involvement, carditis, and dermatological involvement, in which the cumulative prevalence is up to 30%.157
The treatment of pain in inflammatory bowel disease depends on presentation. Antidepressants and opioids should be considered for flares of visceral pain, although chronic opioid use could paradoxically worsen abdominal pain. Given the high co-prevalence rates of depression, anxiety, and other psychiatric illnesses, psychotherapy can be considered.158 Systematic reviews have found evidence for antibiotics in both Crohn’s disease and ulcerative colitis, but paradoxically, the use of antibiotics in childhood could increase the risk for future inflammatory bowel disease.159 160 Immunomodulatory drugs such as azathioprine, methotrexate, and tumor necrosis factor alpha inhibitors have shown effectiveness.161
Myalgic encephalomyelitis or chronic fatigue syndrome
Myalgic encephalitis or chronic fatigue syndrome is a poorly understood clinical condition characterized by post-exertional malaise lasting at least six months, associated with variable symptoms of neurological, immune, endocrine, or autonomic dysfunction.20 162 163 The diagnosis is controversial, with no universally accepted diagnostic criteria.164 The term "chronic fatigue syndrome" was originally proposed as an alternative to "chronic Epstein-Barr syndrome" to describe the symptom complex of chronic fatigue presenting with other (often painful) symptoms, including sore throat, lymph node pain and tenderness, headache, myalgia, and arthralgias.165 Myalgic encephalomyelitis refers to a specific neuro-immunological condition, and has been suggested to be clinically distinct from chronic fatigue syndrome,166 but most practitioners use the two terms synonymously or in combination.163 Although painful symptoms were prominent in earlier case definitions of chronic fatigue syndrome,165 167 more recent clinical diagnostic criteria have de-emphasized pain, which is not required for diagnosis.20 168 Nevertheless, pain remains a common symptom in patients with myalgic encephalitis or chronic fatigue syndrome, and many nociplastic pain conditions (eg, fibromyalgia, temporomandibular disorder, irritable bowel syndrome, migraine) are comorbidities.162
No single cause has been identified for myalgic encephalitis or chronic fatigue syndrome, but immunological, psychological, neurobiological, neuroendocrine, genetic or epigenetic, circulatory, and infectious cause are the most commonly proposed categories, with viral infections implicated in up to 50% of cases in some studies.17 169 170 In some instances, categories can overlap, for example, infectious diseases leading to autoimmune mechanisms. Myalgic encephalitis or chronic fatigue syndrome often presents sporadically, but outbreaks do occur, often in association with viral-like illnesses, suggesting infection as a possible trigger.17 Various epidemiological studies have associated the disorder with Epstein-Barr virus, cytomegalovirus, human herpes viruses 6 or 8, parvovirus B19, enteroviruses, lentivirus, and bacteria such as mycoplasma, Borrelia species, and Coxiella burnetii.17 Covid-19 infection has been associated with the development of prolonged symptoms similar to those found in myalgic encephalitis or chronic fatigue syndrome.171
Infection can trigger an autoreactive process in susceptible individuals, leading to autoimmune responses against energy metabolic processes in the brain and muscle.170 Cytokine signatures have also been causally linked to illness severity of myalgic encephalitis or chronic fatigue syndrome,172 and infection both inside and outside the brain could cause increased production of proinflammatory cytokines, leading to immune mediated dysfunction of the nervous system and energy metabolism.173 Given these proposed relations, use of antiviral and immunomodulatory drugs has been suggested to treat the disorder, but such use is off-label.174 Antiviral drugs such as acyclovir, valacyclovir, and rintatolimod appear to have limited efficacy in treating myalgic encephalitis or chronic fatigue syndrome and can be considered in patients who are seropositive for specific viruses, but evidence is limited by flawed study design and conflicting results.175 Immunomodulatory drugs including corticosteroids, cyclophosphamide, and rituximab have failed to show broad benefit in patients with myalgic encephalitis or chronic fatigue syndrome.175 176 These studies highlight the heterogeneous nature of the disorder and emphasize the importance of developing multimodal, precision medicine approaches to treatment.175 176
Effects of antimicrobial treatment on chronic pain
Chronic pain after infection could be due to numerous causes, so mixed results from studies evaluating antimicrobial treatment are not surprising. Conceptually, whereas antimicrobial treatment should alleviate pain from active inflammatory processes, it should have minimal effects on chronic pain resulting from central sensitization, irrevocable tissue (eg, arthropathy, vasculitis) or nerve injury, or ongoing immune reactions in the absence of detectable pathogen levels (table 3).
Reviews of antibiotic treatment for pain conditions
Psychological implications of infection and chronic pain
Patients with infection can experience biological, psychological, and social stressors that trigger or exacerbate acute pain, leading to chronic pain.5 Psychological factors such as anxiety, depression, and adverse life events are risk factors for the development of chronic pain after infections.177–180 In turn, pain could contribute to the development of mental health comorbidities, yielding a bidirectional association.181 182
Low psychological wellbeing before or during an infection is a risk factor for intestinal disorders after infection, such as irritable bowel syndrome and functional dyspepsia.178–180 183 184 Stress, anxiety, and depression during an episode of acute enteritis, as well as negative life events prior to infection, could be associated with a higher risk of developing irritable bowel syndrome.177 179 183 184 In patients with HIV associated polyneuropathy, mental health is a risk factor for neuropathic pain.185 186 Patients with concurrent depression experience painful HIV neuropathy more frequently than patients without depression, and depressive symptoms are more severe in patients with painful HIV neuropathy than in patients with non-painful neuropathy.185
Post-infectious chronic pain can lead to psychological and social consequences such as anxiety, depression, and poor mental health.187 For example, in one cross sectional study, half of patients with SARS experienced persistent psychological symptoms, despite few having a history of psychiatric illness, with the most common diagnoses being post-traumatic stress disorder and depression.187 In one prospective study, the presence of depression at one month after covid-19 infection predicted persistent pain at three months.188
Because chronic pain, fatigue, sleep disorders, and cognitive difficulties are concurrent in post-infectious syndromes, it can be difficult to infer cause and effect, and these relationships are probably interdependent. One consistent finding across studies is a clear association between chronic pain after infection and poorer quality of life.180–182
Emerging studies
Further research is needed regarding the precise mechanisms by which infections can lead to chronic pain, and whether any of these processes might be therapeutic targets. However, a lack of ongoing studies answers these questions. Between the International Standard Randomised Controlled Trial Number and ClinicalTrials.gov databases, only four ongoing clinical trials pertain to infection and chronic pain. Two trials are observational, with one aiming to identify risk factors for the development of chronic pain after covid-19 infection (NCT04883216), and the other assessing whether covid-19 infection is associated with glycomic or glycan profile changes that might predispose individuals to chronic pain (NCT04788433). The two remaining trials focus on specific interventions. One randomized controlled trial is assessing whether tai chi or health coaching can improve analgesia and quality of life in patients with chronic HIV associated pain (NCT05055596), and one open label prospective trial is assessing whether oral valacyclovir can improve pain and quality of life in patients with Epstein-Barr virus who have interstitial cystitis or bladder pain syndrome (NCT05094414). The NCT05094414 study is the only one among these four that aims to elucidate a specific cause of chronic pain (Epstein-Barr virus) along with a corresponding treatment (valacyclovir). Given the global pervasiveness of chronic pain secondary to infections and its potentially debilitating effects on individuals and communities, this topic deserves greater attention.
Conclusions
Chronic pain is an under-recognized result of infection and might take many forms including nociceptive, neuropathic, and nociplastic pain. Chronic pain can complicate infection by many mechanisms, including direct microbe invasion, immunological processes, treatment toxicity, and psychological triggers. For most chronic pain conditions that develop after infection, treatment is empirical, with antimicrobial agents providing minimal benefit in the absence of evidence for persistent infection. Similar to preventing the transition from acute to chronic pain for other causes, early treatment through a biopsychosocial framework could prevent chronic pain syndromes after infection, although more research is necessary.
Questions for future research
Are there any biomarkers or phenotypes that can identify people with infection who are at higher risk for developing chronic pain, and what steps can be taken to prevent acute pain transitioning into chronic pain?
Can any safe and efficient interventions be given pre-emptively before common infections in patients at high risk for long term adverse consequences including chronic pain?
Does infection independently cause chronic pain, accelerate or accentuate the natural course of nociception (eg, unmask an ongoing process), or exacerbate psychological processes (eg, depression, anxiety) that predispose patients with acute injury to develop chronic pain? How can these related processes be distinguished?
What role do genetics and socioeconomic factors have in the persistence of pain after infection?
Does vaccination or early and aggressive treatment alter the natural course of long term sequelae, including pain after infection?
Patient involvement
Patients were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
References
Footnotes
Contributors SPC: Outline, drafting manuscript, tables, figure, critical review of manuscript. EJW: Drafting manuscript, tables, critical review of manuscript. TLD: Drafting manuscript, critical review of manuscript. LV: Drafting manuscript, critical review of manuscript. KAC: Drafting manuscript, critical review of manuscript. NT: Drafting manuscript, figure, critical review of manuscript. Guarantor: SPC.
Funding Funded in part by a grant from MIRROR, Uniformed Services University of the Health Sciences, US Department of Defence (grant HU00011920011). The sponsor did not have a role in study design or performance, or analysis or interpretation of data.
Competing interests We have read and understood the BMJ policy on declaration of interests and declare the following interests: SPC has undertaken consultant work for Releviate, SPR Therapeutics, Avanos, Persica, and Scilex; and conducted institutional research funded by Scilex and Avanos.
Provenance and peer review Commissioned; externally peer reviewed.